
Anti-CCP Antibody Test
Anti-CCP Antibody Test Explained: A Laboratory Medicine Specialist’s Guide to Rheumatoid Arthritis Diagnosis
Introduction
This article is written by a Laboratory Medicine Specialist (MD.phD.) with clinical expertise in autoimmune serology, immunoassay diagnostics, and rheumatological laboratory evaluation.
The Anti-CCP antibody test (anti-cyclic citrullinated peptide antibody) is one of the most diagnostically powerful tools available for the early detection and prognostic evaluation of rheumatoid arthritis (RA) — a chronic, systemic autoimmune disease affecting millions of people worldwide. With a specificity approaching 95–98%, it significantly outperforms the traditional rheumatoid factor (RF) test in ruling in RA, and it can turn positive years before clinical symptoms fully emerge. In this post, we cover what Anti-CCP is, how it is measured, how to interpret results, and what a positive or negative finding means for patients and clinicians.
What Is the Anti-CCP Antibody Test and What Is Its Purpose?
Defining the Test
The Anti-CCP antibody test detects autoantibodies directed against cyclic citrullinated peptides (CCPs) — synthetic peptides that mimic citrullinated proteins found in inflamed joint tissue. Citrullination is a post-translational protein modification in which the amino acid arginine is enzymatically converted to citrulline. In healthy individuals, this process is regulated and limited; in patients with rheumatoid arthritis, citrullination occurs aberrantly and extensively within the synovium, triggering an autoimmune response.
The resulting autoantibodies — Anti-CCP antibodies — are highly specific to RA and can be detected in serum years before the onset of joint damage, making them an exceptionally valuable early biomarker.
Pathophysiological Mechanism
In RA, the enzyme peptidylarginine deiminase (PAD) — particularly the PAD4 isoform — is overactivated in the synovial microenvironment, generating an abundance of citrullinated proteins such as fibrinogen, vimentin, collagen type II, and α-enolase. Genetically susceptible individuals (particularly those carrying the HLA-DRB1 shared epitope) mount an adaptive immune response against these neoantigens, producing Anti-CCP antibodies. These antibodies contribute directly to synovial inflammation and osteoclast activation, accelerating joint erosion.
Clinical Indications: When Is This Test Ordered?
Clinicians order the Anti-CCP antibody test in the following situations:
- Suspected early rheumatoid arthritis — particularly when symptoms are nonspecific (morning stiffness, symmetric small joint pain)
- Differentiation of RA from other inflammatory arthropathies (psoriatic arthritis, lupus arthritis, reactive arthritis)
- RF-seronegative patients with clinical features consistent with RA
- Assessment of disease prognosis and erosive potential at diagnosis
- Evaluation of undifferentiated inflammatory arthritis to guide treatment decisions
Reference Ranges for Anti-CCP Antibody
The Anti-CCP antibody test is most commonly performed using CMIA (Chemiluminescent Microparticle Immunoassay), an automated, high-throughput immunochemical method that offers excellent sensitivity, specificity, and reproducibility. Results are reported in U/mL (units per milliliter).
| Result Category | Threshold | Interpretation |
|---|---|---|
| Negative | < 5.0 U/mL | Anti-CCP antibodies not detected; RA less likely but not excluded |
| Positive | ≥ 5.0 U/mL | Anti-CCP antibodies detected; associated with RA |
| Weakly Positive | 5.0 – 10.0 U/mL* | Low-titer positivity; requires correlation with clinical findings |
| Strongly Positive | > 10.0 U/mL* | Higher specificity for RA; associated with more aggressive disease course |
Titer sub-categorization thresholds vary by reagent manufacturer and laboratory platform.
⚠️ Important: Reference ranges vary between laboratories and assay systems. Always interpret results using the reference range established by the performing laboratory. Do not compare values across different platforms or institutions without verification.
About the CMIA Method
| Feature | Detail |
|---|---|
| Method | Chemiluminescent Microparticle Immunoassay (CMIA) |
| Automation | Fully automated; suitable for high-volume labs |
| Turnaround time | Rapid (typically same-day or next-day) |
| Reproducibility | Excellent inter- and intra-assay precision |
| Common platforms | Abbott ARCHITECT, Siemens ADVIA Centaur |
Clinical Interpretation of Anti-CCP Antibody Results
Positive Results (Elevated Anti-CCP)
A positive Anti-CCP result carries significant diagnostic and prognostic weight. The following conditions and clinical contexts are associated with Anti-CCP positivity:
Primary association — Rheumatoid Arthritis:
- Early RA — Anti-CCP positivity may precede clinical diagnosis by 5–10 years, enabling pre-symptomatic identification in high-risk individuals
- RF-seronegative RA — Anti-CCP fills a critical diagnostic gap in the approximately 20–30% of RA patients who test negative for rheumatoid factor
- Erosive RA — Anti-CCP–positive patients demonstrate significantly higher rates of radiographic joint erosion and more rapid structural deterioration than seronegative counterparts
- Aggressive disease phenotype — Positivity correlates with more severe synovitis, greater functional impairment, and poorer long-term joint outcomes
Non-RA conditions where low-titer positivity may occur:
- Chronic tuberculosis (TB) — via citrullination in granulomatous tissue
- Chronic obstructive pulmonary disease (COPD) and other chronic lung diseases
- Systemic lupus erythematosus (SLE)
- Sjögren’s syndrome
- Juvenile idiopathic arthritis (in a subset of patients)
Conditions associated with false-positive results (typically low titer):
- Behçet’s disease
- Fibromyalgia
- Gout (crystal arthropathy)
- Osteoarthritis
Mechanistic note: In non-RA conditions, citrullination can occur as a nonspecific consequence of inflammation or cellular death. However, the magnitude of the immune response against citrullinated peptides is far lower than in true RA, which is why titers in these settings tend to be weak.
Negative Results (Low or Undetectable Anti-CCP)
A negative Anti-CCP result does not exclude rheumatoid arthritis. The following scenarios should be considered:
- Early or pre-clinical RA — seroconversion may not yet have occurred; repeat testing in 6–12 months may be warranted if clinical suspicion remains
- Seronegative RA — a well-recognized RA subset that is Anti-CCP and RF negative but clinically and histologically indistinguishable from seropositive disease
- Undifferentiated inflammatory arthritis — may evolve into RA, psoriatic arthritis, or resolve spontaneously; longitudinal monitoring is required
- Alternative diagnoses — reactive arthritis, viral arthritis (parvovirus B19, hepatitis B/C), crystal arthropathy, or connective tissue disease with joint involvement
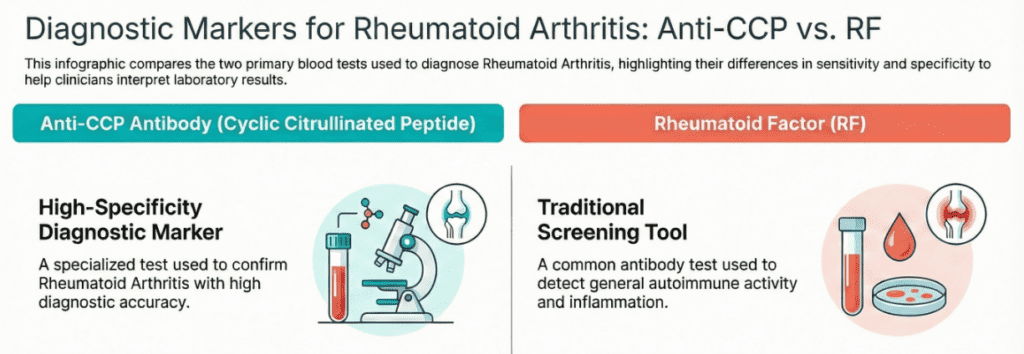
Diagnostic Performance: Sensitivity and Specificity
| Parameter | Anti-CCP Antibody | Rheumatoid Factor (RF) |
|---|---|---|
| Sensitivity | ~70–80% | ~60–70% |
| Specificity | ~95–98% | ~70–80% |
| Positive Predictive Value | Very high | Moderate |
| False-positive rate | Very low | Higher |
| Detection before symptoms | Yes (years earlier) | Less reliable |
The critical clinical implication of this data: a positive Anti-CCP result is highly confirmatory, while a negative result does not rule out RA. This asymmetry shapes how the test should be used — as a powerful rule-in tool rather than a screening instrument for low-prevalence populations.
Dual testing strategy: Ordering Anti-CCP and RF simultaneously increases diagnostic accuracy beyond either test alone. A patient who is both RF-positive and Anti-CCP-positive carries a very high probability of RA and is at elevated risk for aggressive, erosive disease.
Precautions and Limitations
Several factors may influence Anti-CCP test results or complicate their interpretation:
Pre-analytical variables:
- No specific fasting requirement, but sample hemolysis or prolonged storage can affect immunoassay performance
- Results should be interpreted alongside the patient’s complete clinical picture, not in isolation
Analytical considerations:
- Different laboratory platforms (CMIA, ELISA, multiplex bead assays) may yield non-equivalent numerical results — direct comparison across labs is unreliable
- The CCP antigen generation used (CCP2, CCP3) affects assay performance; most modern clinical laboratories use second- or third-generation assays
Clinical limitations:
- Anti-CCP is a diagnostic and prognostic marker, not a disease activity monitor — it does not reliably rise and fall with RA flares or treatment response
- A positive result alone is never sufficient to diagnose RA without corroborating clinical, imaging (X-ray, MRI, musculoskeletal ultrasound), and additional serological data
- Low-titer positivity in the context of non-RA diagnoses (TB, SLE, chronic lung disease) can be misleading if clinical context is not considered
Patient counseling note: Patients should be advised that a positive Anti-CCP does not automatically mean they have RA, and a negative result does not mean they do not. These results are one data point within a comprehensive diagnostic evaluation, and a rheumatologist’s clinical assessment remains indispensable.
Specialist’s Perspective and Conclusion
In my experience in laboratory medicine and autoimmune diagnostics, the Anti-CCP antibody test represents one of the most clinically meaningful advances in rheumatological serology of the past two decades. Before its widespread adoption, diagnosing RA early — particularly in RF-seronegative patients — was a substantial clinical challenge. Anti-CCP changed that calculus dramatically.
What I find most clinically important to communicate is the asymmetric diagnostic logic of this test: a strong positive, especially at high titer, is powerful evidence in favor of RA and should prompt urgent rheumatological referral; a negative result, however, carries limited reassurance in a patient with convincing clinical features. In that setting, repeat testing, imaging, and specialist review remain essential.
I also want to emphasize a point that laboratory results alone cannot convey: Anti-CCP-positive patients face a fundamentally different disease trajectory than their seronegative counterparts. Early, aggressive treatment in seropositive patients — ideally with disease-modifying antirheumatic drugs (DMARDs) before radiographic erosion appears — is one of the most impactful interventions in modern rheumatology. The laboratory finding should activate a clinical response, not simply be filed in a chart.
Key takeaway: The Anti-CCP antibody test is a high-specificity, early-detection tool that plays a central role in RA diagnosis and prognosis. Used appropriately — in combination with RF, clinical assessment, and imaging — it gives clinicians and patients a meaningful head start against one of the most common and potentially disabling autoimmune diseases.
Author Profile
The author is a board-certified physician specializing in Laboratory Medicine, with focused expertise in clinical immunology, autoimmune serology, and diagnostic test evaluation. With experience spanning hospital-based diagnostic laboratories and medical content development, they are committed to translating complex laboratory science into clinically actionable, globally accessible knowledge.
https://medlabinsight.com/spot-exams-in-medical-school/
References
- Aletaha, D., Neogi, T., Silman, A. J., et al. (2010). 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis & Rheumatism, 62(9), 2569–2581. https://doi.org/10.1002/art.27584
- Schellekens, G. A., de Jong, B. A., van den Hoogen, F. H., et al. (1998). Citrulline is an essential constituent of antigenic determinants recognized by rheumatoid arthritis-specific autoantibodies. Journal of Clinical Investigation, 101(1), 273–281. https://doi.org/10.1172/JCI1316
- van Venrooij, W. J., van Beers, J. J., & Pruijn, G. J. (2011). Anti-CCP antibodies: The past, the present and the future. Nature Reviews Rheumatology, 7(7), 391–398. https://doi.org/10.1038/nrrheum.2011.76
- Nishimura, K., Sugiyama, D., Kogata, Y., et al. (2007). Meta-analysis: Diagnostic accuracy of anti-cyclic citrullinated peptide antibody and rheumatoid factor for rheumatoid arthritis. Annals of Internal Medicine, 146(11), 797–808. https://doi.org/10.7326/0003-4819-146-11-200706050-00008
- Mayo Clinic Laboratories. Anti-Cyclic Citrullinated Peptide (Anti-CCP) Antibody, IgG, Serum. https://www.mayocliniclabs.com
- Smolen, J. S., Aletaha, D., Barton, A., et al. (2018). Rheumatoid arthritis. Nature Reviews Disease Primers, 4, 18001. https://doi.org/10.1038/nrdp.2018.1
- UpToDate. Diagnosis and differential diagnosis of rheumatoid arthritis. Wolters Kluwer. https://www.uptodate.com