
Osteology Explained: A Specialist’s Guide
Osteology Explained: A Specialist’s Guide to the Science of Bone
Introduction
This article is written by a Laboratory Medicine Specialist and medical educator with extensive experience in anatomical sciences and clinical medicine.
Osteology — from the Greek osteon (bone) and logos (study) — is the systematic study of bones, and it forms the absolute foundation of medical education. Far from being a simple memorization exercise, osteology is an applied science that underpins surgery, radiology, emergency medicine, dentistry, and pediatric care. In this post, we explore what osteology is, why it matters clinically, and how a deep understanding of the skeletal system unlocks nearly every domain of modern medicine.
What Is Osteology and What Does It Cover?
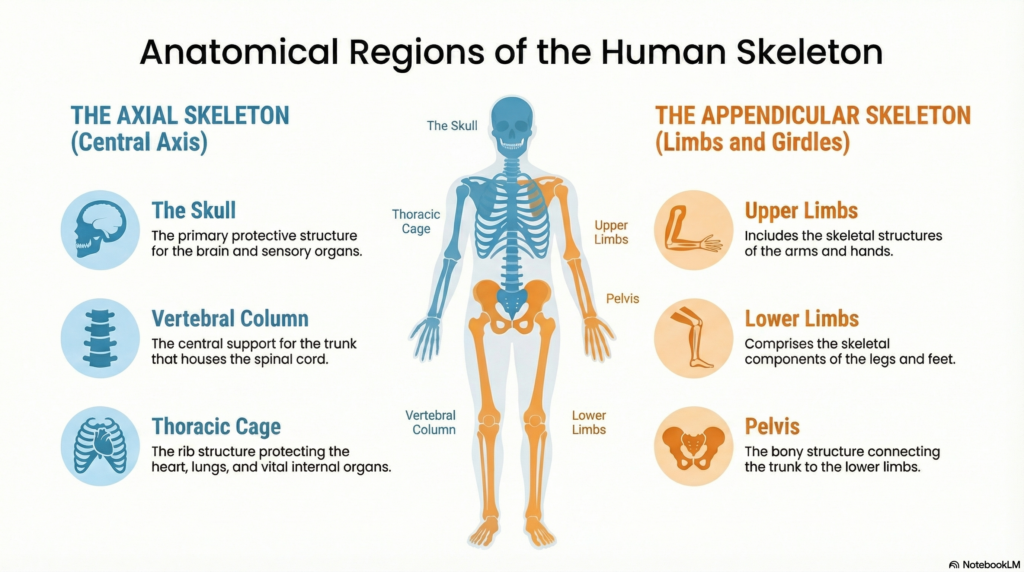
Osteology is a subdiscipline of anatomy concerned with the structure, function, development, and surface landmarks of the 206 bones that comprise the adult human skeleton. It is far more than naming bones — it is understanding how they are built, how they grow, how they connect, and how they interact with surrounding nerves, vessels, and organs.
Core Areas of Study
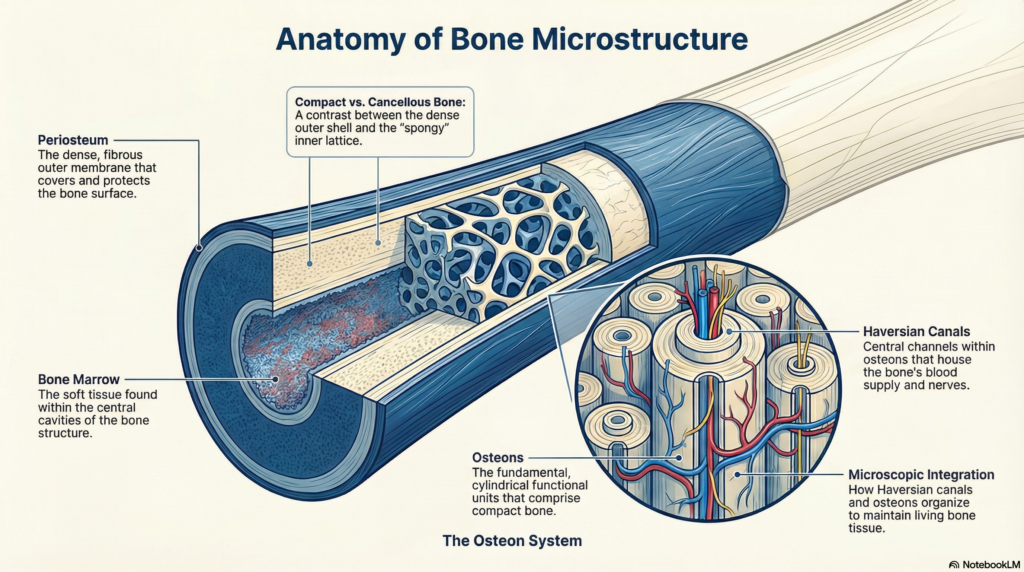
Bone Structure Each bone is a living organ composed of compact (cortical) bone on its exterior and cancellous (spongy) bone internally. The periosteum (outer membrane) carries blood vessels and nerves, while the medullary cavity houses bone marrow. Understanding this architecture is essential before any surgical incision.
Ossification (Bone Development) Bones form through two primary mechanisms:
- Endochondral ossification — the replacement of a cartilage template by bone tissue (e.g., long bones of the limbs)
- Intramembranous ossification — direct mineralization of connective tissue (e.g., flat bones of the skull)
The epiphyseal (growth) plate is a critical structure in pediatrics; its premature closure leads to growth disorders.
Surface Anatomy (Bony Landmarks) Osteology maps projections (processes), ridges (crests), bumps (tubercles, tuberosities), openings (foramina), and grooves (sulci) — all of which serve as guides for clinicians identifying nerve pathways, injection sites, and surgical entry points.
Articulation (Joint Relationships) How bones meet determines joint type and range of motion. Osteology integrates with arthrology (joint science) to explain why a ball-and-socket hip joint allows multiaxial movement while a hinge joint at the elbow does not.
Functional Roles of Bone
| Function | Example |
|---|---|
| Mechanical support | Vertebral column supports upright posture |
| Locomotion | Femur transmits force during walking |
| Mineral reservoir | 99% of body calcium stored in bone |
| Hematopoiesis | Red blood cells produced in red marrow |
| Organ protection | Skull protects the brain; rib cage shields lungs and heart |
Normal Reference: The Adult Human Skeleton at a Glance
| Region | Number of Bones | Clinical Notes |
|---|---|---|
| Skull (cranium + facial) | 22 | Complex foramina; houses cranial nerves |
| Vertebral column | 33 (26 functional) | C1–C7, T1–T12, L1–L5, Sacrum, Coccyx |
| Thoracic cage (ribs + sternum) | 25 | 12 pairs of ribs; protects cardiothoracic organs |
| Upper limb (each side) | 32 | Scapula, clavicle, humerus, radius, ulna, carpals, metacarpals, phalanges |
| Lower limb (each side) | 31 | Femur, patella, tibia, fibula, tarsals, metatarsals, phalanges |
| Pelvic girdle | 2 (hip bones) | Each formed by fusion of ilium, ischium, pubis |
Note: Bone count can vary slightly between individuals due to sesamoid bones, sutural (Wormian) bones in the skull, or anatomical variants. The standard adult count is 206.
Clinical Importance: Why Every Doctor Must Know Osteology
Orthopedic and Neurosurgical Applications
Fracture reduction, internal fixation with plates and screws, joint replacement, and spinal decompression are all impossible without detailed knowledge of skeletal anatomy. A surgeon must know the exact shape of a vertebral pedicle before placing a pedicle screw to avoid spinal cord injury.
Radiological Interpretation (X-ray, CT, MRI)
Radiologists and clinicians must identify bony landmarks to localize pathology precisely. Descriptions like “L4–L5 disc herniation compressing the right L5 nerve root” or “nondisplaced fracture of the femoral neck” are only meaningful with solid osteological grounding.
Emergency and Trauma Medicine
In polytrauma, rapid identification of fracture patterns guides triage:
- Rib fractures → risk of pneumothorax or hemothorax
- Pelvic ring disruption → risk of massive retroperitoneal hemorrhage
- C-spine fractures → risk of spinal cord injury
Dentistry and Maxillofacial Surgery
Mandibular and maxillary bone morphology dictates implant placement depth, orthodontic bracket positioning, and the extent of corrective jaw osteotomies. Facial growth patterns must be understood before any surgical intervention in children.
Pediatric Growth Assessment
The epiphyseal plate (growth plate) is visible on plain X-rays in skeletally immature patients. Bone age assessment — comparing skeletal maturation against chronological age — is a standard tool for evaluating growth hormone deficiency, precocious puberty, and nutritional status.
Key Bones and Regions in Osteology Education
1. The Skull
The 22 bones of the skull — including the frontal, parietal, temporal, and occipital bones — form a complex interlocking structure that protects the brain while housing the organs of special sense. Multiple foramina transmit the 12 cranial nerves.
2. The Vertebral Column
The 33 vertebrae (functionally 26) are organized into five regions. The intervertebral foramina transmit spinal nerves; stenosis at these points causes radiculopathy — one of the most common pain syndromes in clinical practice.
3. The Thoracic Cage
Twelve pairs of ribs articulate posteriorly with thoracic vertebrae. The upper seven (“true ribs”) attach directly to the sternum; ribs 8–10 attach via costal cartilage; ribs 11–12 are “floating.” This anatomy determines respiratory mechanics and the approach to chest tube insertion.
4. Upper and Lower Limbs
Long bone anatomy — shaft (diaphysis), ends (epiphyses), metaphysis — is fundamental to understanding fracture classification and healing. The proximal femur, in particular, is the most clinically significant bone in orthopedics due to the frequency and morbidity of hip fractures.
5. The Pelvis
Formed by the fusion of the ilium, ischium, and pubis at the acetabulum, the pelvis distributes axial load to the lower limbs, provides attachment for core muscles, protects pelvic viscera, and — in females — forms the birth canal.
Precautions and Limitations in Applied Osteology
- Individual anatomical variation is common. Accessory ossicles, bipartite bones (e.g., bipartite patella), and unfused apophyses can mimic fractures on imaging.
- Age-related changes (osteoporosis, osteophyte formation) alter normal landmarks; what is normal at 30 may be pathological at 70.
- Imaging modality matters. Plain X-rays show cortical bone well but miss early stress fractures and soft tissue injury. MRI is superior for bone marrow pathology. CT provides the best 3D bony detail.
- Clinical context is essential. A single X-ray or anatomical finding should never be interpreted in isolation. Always correlate with patient history, physical examination, and laboratory results.
- Pediatric vs. adult skeletons differ fundamentally. Open growth plates, cartilaginous epiphyses, and more elastic bone in children change how injuries present and how they are managed.
Specialist’s Perspective and Conclusion
Having worked at the interface of laboratory medicine and clinical anatomy, I can affirm that osteology is not a passive knowledge base — it is an active clinical toolkit. Every time a clinician orders a bone mineral density scan, interprets a skeletal survey for multiple myeloma, or evaluates a bone marrow biopsy, they are drawing on osteological principles.
What makes osteology particularly powerful is its integrative nature. Understanding bone structure leads naturally to understanding joint mechanics, muscle attachment, nerve pathways, and vascular territories. It is genuinely the entry point into the full map of human anatomy.
Key takeaway: Master osteology, and you hold the architectural blueprint of the human body. Every specialty — from neurosurgery to emergency medicine to dentistry — speaks the language of bone.
Author Profile
The author is a board-certified physician with specialization in Laboratory Medicine and a background in anatomical sciences and medical education. With experience spanning clinical diagnostics, academic teaching, and medical content development, they write to make complex biomedical knowledge accessible, accurate, and actionable for a global audience.
https://medlabinsight.com/body-fluid-analysis-interpretation-guide/
References
Resnick, D., & Kransdorf, M. J. (2005). Bone and Joint Imaging (3rd ed.). Elsevier Saunders.
Drake, R. L., Vogl, A. W., & Mitchell, A. W. M. (2020). Gray’s Anatomy for Students (4th ed.). Elsevier.
Moore, K. L., Dalley, A. F., & Agur, A. M. R. (2018). Clinically Oriented Anatomy (8th ed.). Wolters Kluwer.
Standring, S. (Ed.). (2021). Gray’s Anatomy: The Anatomical Basis of Clinical Practice (42nd ed.). Elsevier.
Netter, F. H. (2019). Atlas of Human Anatomy (7th ed.). Elsevier.
National Institutes of Health (NIH) — National Institute of Arthritis and Musculoskeletal and Skin Diseases. Bone Health and Osteoporosis. https://www.niams.nih.gov