
[MD.phD.] Eosinophil Count Test
Eosinophil Count Test: A Laboratory Medicine Specialist’s Complete Guide to Interpretation
The eosinophil count is a fundamental blood test that measures a specific white blood cell involved in allergic and parasitic responses. This guide covers what the test measures, how to interpret elevated or low results, normal reference ranges, and the critical pre-analytical factors that can compromise accuracy.
Written by a Laboratory Medicine Specialist (MD.phD.)
Board-certified physician with expertise in clinical hematology, flow cytometric analysis, and laboratory diagnostics. This article is intended for educational purposes for clinicians and informed patients.
Introduction
Among the five types of white blood cells routinely measured in a complete blood count (CBC), eosinophils occupy a uniquely important role in immune defense — particularly against parasitic infections and type 2 inflammatory responses. As a laboratory medicine specialist, I frequently see eosinophil counts ordered as a first-line investigation, yet the results are often misread or their limitations misunderstood.
In this guide, I walk through everything a clinician — or an informed patient — needs to know: what eosinophils do, when their count rises or falls, how to interpret the numbers, and what analytical pitfalls to watch for.
Key takeaway: An elevated eosinophil count (eosinophilia) is not a diagnosis — it is a laboratory signal pointing toward a differential that includes parasitic infection, atopic disease, drug hypersensitivity, or, less commonly, hematologic malignancy.
What Is the Eosinophil Count Test and Why Is It Ordered?
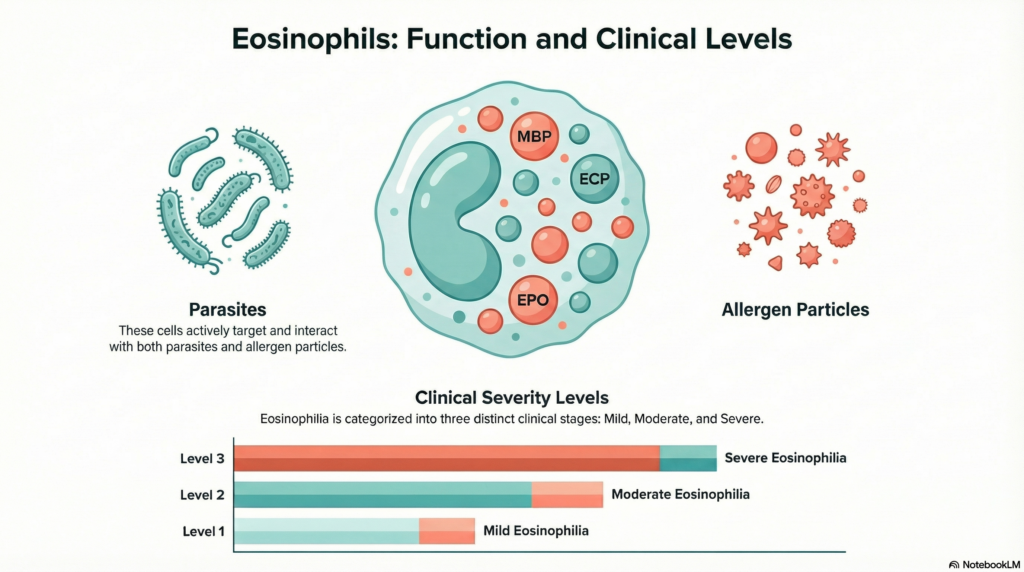
Eosinophils are granulocytic leukocytes — white blood cells packed with large cytoplasmic granules that stain intensely with the acidic dye eosin, giving them their name. They are produced in the bone marrow and circulate in the blood for roughly 8–12 hours before migrating to tissues, where they can persist for days.
The eosinophil count test measures both the percentage of eosinophils among all white blood cells (relative count, %) and their absolute number per microliter of blood (absolute eosinophil count, AEC). Both values are reported automatically as part of the differential white cell count on modern hematology analyzers.
Clinical indications — when is this test ordered?
- Evaluation of suspected parasitic infections (especially tissue-invasive helminths)
- Work-up of allergic or atopic conditions: asthma, allergic rhinitis, atopic dermatitis
- Monitoring disease activity in known eosinophilic disorders
- Investigation of unexplained peripheral blood eosinophilia detected incidentally
- Suspected drug hypersensitivity reactions (e.g., DRESS syndrome)
- Evaluation of potential eosinophilic granulomatosis with polyangiitis (EGPA)
- Screening during assessment of adrenal insufficiency
Normal Reference Ranges
Reference intervals are established for healthy adult populations. Pediatric values are similar but should be verified against age-specific laboratory norms.
| Parameter | Normal Range | Unit | Clinical Significance |
|---|---|---|---|
| Eosinophils (relative) | 0 – 6% | % of WBC differential | Normal |
| Absolute Eosinophil Count (AEC) | 50 – 500 | /µL (cells per microliter) | Normal |
| Mild eosinophilia | 500 – 1,500 | /µL | Mild ↑ |
| Moderate eosinophilia | 1,500 – 5,000 | /µL | Moderate ↑ |
| Severe (hypereosinophilia) | > 5,000 | /µL | Severe ↑ |
* Reference ranges may vary slightly by laboratory and analyzer platform. Always interpret results in context of your institution’s reference interval. The clinically critical threshold for potential end-organ damage is a sustained AEC above 1,500/µL.
Important clinical threshold: An AEC persistently above 1,500/µL warrants systematic evaluation for hypereosinophilic syndrome (HES) and monitoring for cardiac, pulmonary, and neurological complications from eosinophil-mediated tissue injury.
How the Test Is Performed: Flow Cytometry on Automated Analyzers

Modern clinical laboratories perform the eosinophil count using automated hematology analyzers that employ flow cytometry or impedance-based differential leukocyte counting. Here is how it works:
- Laser interrogation: Cells pass single-file through a laser beam. Light scatter patterns are captured simultaneously.
- Forward scatter (FSC) correlates with cell size; side scatter (SSC) reflects internal granularity. Eosinophils have characteristically high SSC due to their large, abundant granules.
- Automated classification: The analyzer plots cells on a scattergram and uses gating algorithms to enumerate each leukocyte population — including eosinophils — producing both the absolute count and percentage.
- In complex or flagged specimens, a trained medical laboratory scientist performs a manual differential on a stained peripheral blood smear to confirm results.
This technology allows thousands of cells to be analyzed per second, delivering results typically within minutes of sample receipt.
Clinical Interpretation: Elevated and Decreased Eosinophils
Interpreting the eosinophil count is never done in isolation — it must be integrated with clinical history, symptoms, travel history, medication list, and other laboratory findings.
High eosinophil count (eosinophilia) — causes and associations
Parasitic Infections
- Toxocara spp. (visceral larva migrans)
- Strongyloides stercoralis
- Ascaris lumbricoides
- Paragonimus (lung fluke)
- Trichinella spiralis
- Filariasis
Allergic & Atopic Disorders
- Bronchial asthma
- Allergic rhinitis
- Atopic dermatitis
- Chronic urticaria
- Drug hypersensitivity (DRESS)
Autoimmune / Vasculitic
- EGPA (Churg-Strauss syndrome)
- Eosinophilic granulomatosis
- Connective tissue diseases
- Inflammatory bowel disease
Hematologic Malignancy
- Eosinophilic leukemia (CEL-NOS)
- Myeloproliferative neoplasms
- Hodgkin lymphoma
- AML subtypes (M4eo)
Gastrointestinal
- Eosinophilic esophagitis
- Eosinophilic gastroenteritis
- Eosinophilic colitis
Endocrine / Other
- Primary adrenal insufficiency
- Hypopituitarism
- Post-splenectomy state
- Solid organ transplant rejection
Mechanistic note: In parasitic infections, eosinophilia is driven by IL-5 released from T helper 2 (Th2) lymphocytes. Eosinophils are recruited to tissues where their granule proteins — including Major Basic Protein (MBP) and Eosinophil Cationic Protein (ECP) — exert direct cytotoxicity against helminths.
Low eosinophil count (eosinopenia) — causes
Eosinopenia is less clinically significant than eosinophilia, but its presence can be informative in certain contexts:
Endogenous / Physiologic
- Acute physiologic stress response
- Post-surgical states
- Cushing syndrome (cortisol excess)
- Diurnal variation (morning nadir)
Pharmacologic / Iatrogenic
- Systemic corticosteroid therapy
- Epinephrine administration
- Immunosuppressive regimens
- Sepsis (early phase)
Corticosteroids suppress eosinophil production and accelerate their apoptosis — a finding that is frequently exploited therapeutically in allergic and eosinophilic conditions.
Precautions and Analytical Limitations
In my experience, pre-analytical and analytical errors account for many unexpected or erroneous eosinophil results. Understanding these limitations is essential for both the ordering clinician and the laboratory team.
1. Adequate sample mixing is the single most important pre-analytical step. EDTA-anticoagulated tubes must be gently inverted 8–10 times immediately after collection. Inadequate mixing causes microclot formation, which distorts all white cell counts and triggers instrument flags requiring recollection.
2. Time to analysis matters. Samples left at room temperature beyond 4–6 hours undergo progressive cell degradation and morphological change. Where possible, analysis within 2–4 hours of venipuncture is recommended to ensure both percentage and absolute count accuracy.
3. Medications significantly affect results. Systemic corticosteroids, epinephrine, and certain immunosuppressants suppress eosinophil counts. Always document current medications when ordering this test and interpret accordingly.
4. Seasonal and allergen-exposure variation. In atopic patients, eosinophil counts may fluctuate with allergen season. A single in-range result does not exclude atopic disease; longitudinal trending is more informative.
5. Absolute count is preferred over percentage alone. The percentage can be misleadingly normal if total WBC is elevated. Always evaluate the absolute eosinophil count (AEC) when assessing eosinophilia severity.
Self-diagnosis warning: A single abnormal eosinophil count is not sufficient to establish any diagnosis. Results must be interpreted by a physician in the full clinical context. Do not attempt to self-diagnose based on laboratory values alone.
Specialist’s Perspective and Clinical Takeaways
In over a decade of laboratory medicine practice, the eosinophil count remains one of the most underappreciated data points on a routine CBC. Clinicians often dismiss mild elevations as insignificant, or over-react to a transient finding driven by poor sample handling. The key is systematic interpretation: sustained elevation above 1,500/µL demands a structured work-up, and pre-analytical quality cannot be an afterthought.
— Laboratory Medicine Specialist, MD.phD.
Here are the key practical takeaways from this guide:
- Always report and interpret the absolute eosinophil count — not just the percentage.
- A sustained AEC above 1,500/µL warrants organ evaluation (cardiac troponin, echocardiography, pulmonary function tests).
- Travel history and potential helminth exposure should be the first question when unexplained eosinophilia is encountered.
- Pre-analytical tube handling is the most controllable variable determining result accuracy — invest in proper phlebotomy training.
- Eosinopenia in the setting of sepsis may carry prognostic significance and should not be entirely dismissed.
About the Author
MD.phD.
The author is a board-certified physician specializing in Laboratory Medicine, with subspecialty expertise in clinical hematology and flow cytometric diagnostics. Their clinical work encompasses the evaluation of hematologic malignancies, coagulation disorders, and complex CBC interpretation. All content in this article is written for educational purposes and reflects evidence-based laboratory medicine practice.
https://medlabinsight.com/body-fluid-analysis-interpretation-guide/
References
- Klion, A. D. (2022). Eosinophilia: Causes and evaluation. UpToDate. Retrieved from uptodate.com
- Ramirez, G. A., Yacoub, M. R., Ripa, M., et al. (2018). Eosinophils from physiology to disease: A comprehensive review. BioMed Research International, 2018, 9095275. https://doi.org/10.1155/2018/9095275
- Mayo Clinic Laboratories. (2024). Eosinophil count: Reference values and clinical interpretation. Retrieved from mayocliniclabs.com
- Gotlib, J. (2023). World Health Organization-defined eosinophilic disorders: 2022 update on diagnosis, risk stratification, and management. American Journal of Hematology, 98(7), 1244–1263. https://doi.org/10.1002/ajh.26950
- Valent, P., Klion, A. D., Horny, H. P., et al. (2012). Contemporary consensus proposal on criteria and classification of eosinophilic disorders and related syndromes. Journal of Allergy and Clinical Immunology, 130(3), 607–612.e9. https://doi.org/10.1016/j.jaci.2012.02.019
- National Institutes of Health — MedlinePlus. (2024). Eosinophil count — absolute. Retrieved from medlineplus.gov