
[MD.phD.] Leukopenia vs Neutropenia
Leukopenia vs. Neutropenia: A Laboratory Medicine Specialist’s Guide to the Key Differences
Leukopenia refers to a total white blood cell count below 4,000/µL, while neutropenia specifically means a low absolute neutrophil count — the single most important predictor of infection risk. Though the two conditions frequently overlap, their clinical implications, severity thresholds, and management strategies are fundamentally different. This guide walks through the definitions, diagnostic criteria, causes, and critical interpretation pitfalls every clinician should know.
Written by a Laboratory Medicine Specialist (MD.phD.)
Board-certified physician specializing in clinical hematology, automated cell analysis, and laboratory-based diagnostic interpretation. All content reflects current evidence-based practice and is intended for educational purposes.
Introduction
When a complete blood count (CBC) comes back with a low white blood cell (WBC) count, the instinct is to flag it and move on. But that single number — the total WBC — tells only part of the story. As a laboratory medicine specialist, one of the most common interpretive errors I encounter in practice is treating a low WBC as interchangeable with a low neutrophil count. They are not the same thing, and conflating them can lead to delayed treatment of a potentially life-threatening infection — or, conversely, unnecessary intervention.
This article draws a clear line between leukopenia (reduced total white cell count) and neutropenia (reduced absolute neutrophil count), explains why the distinction matters clinically, and provides a practical framework for interpreting both conditions accurately.
The core principle: Infection risk in a patient with a low WBC is determined primarily by the absolute neutrophil count (ANC), not the total leukocyte count. Always calculate the ANC before drawing clinical conclusions from a low WBC.
Definitions and Core Distinctions
Before diving into thresholds and causes, it helps to see both conditions side by side:
Leukopenia
A reduction in the total white blood cell count below the laboratory’s lower reference limit — typically <4,000/µL in adults.
vs.
Neutropenia
A reduction in the absolute neutrophil count (ANC) below 1,500/µL — the most infection-relevant component of the white cell differential.
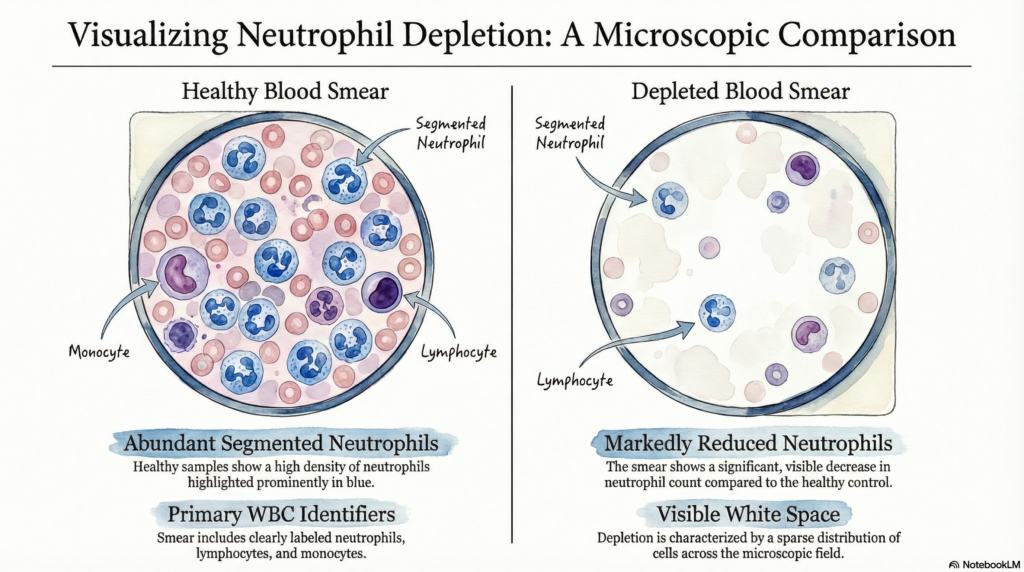
The white blood cell compartment is not homogeneous. It encompasses five major cell types: neutrophils, lymphocytes, monocytes, eosinophils, and basophils. Leukopenia tells you the total army is diminished; neutropenia tells you the frontline infantry is depleted. The latter is what matters most for immediate infection risk.
What is leukopenia?
Leukopenia is defined as a total WBC count below 4,000 cells/µL in most adult reference ranges (some laboratories use 3,500/µL). The term captures any combination of reductions across the leukocyte subtypes. Because any of the five cell types could be responsible for the drop, a low total WBC is an entry-level finding that always requires differential analysis to determine which subpopulation is involved and what the clinical consequences might be.
Leukopenia alone does not reliably predict infection risk. A patient with a WBC of 3,200/µL driven entirely by lymphopenia may have a normal neutrophil count and face minimal near-term infection risk, while a patient with a borderline-low WBC of 3,800/µL dominated by neutropenia may be at serious risk of bacterial or fungal sepsis.
What is neutropenia?
Neutropenia is defined by a reduction in the Absolute Neutrophil Count (ANC) below 1,500/µL. Neutrophils are the primary cellular defense against extracellular bacteria and certain fungi. When their numbers fall, the host’s capacity for phagocytosis and pathogen clearance is compromised in a directly proportional manner.
The ANC is calculated from the CBC differential rather than read directly. The formula is:
ANC = WBC × (% Neutrophils + % Bands) / 100
Bands = immature neutrophils (band forms). Both segmented neutrophils and bands are included.
This calculation is essential. A patient with a WBC of 5,000/µL but only 20% neutrophils has an ANC of 1,000/µL — firmly within the neutropenic range — despite a normal total leukocyte count. The converse is equally possible: leukopenia without neutropenia.
Reference Ranges and Severity Classification
Leukopenia threshold
| Category | WBC Threshold | Unit | Classification |
|---|---|---|---|
| Normal adult WBC | 4,000 – 11,000 | /µL | Normal |
| Leukopenia | < 4,000 | /µL | Low — investigate |
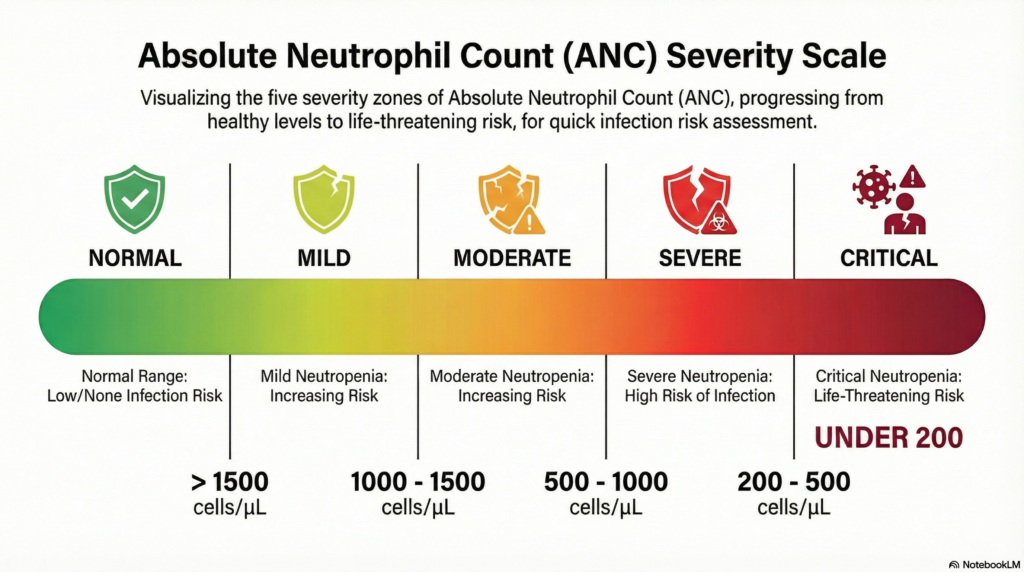
Neutropenia — severity classification
| Severity Grade | ANC Range | Unit | Infection Risk |
|---|---|---|---|
| Normal | 1,500 – 8,000 | /µL | Standard risk |
| Mild neutropenia | 1,000 – 1,500 | /µL | Mildly elevated risk |
| Moderate neutropenia | 500 – 1,000 | /µL | Significant risk |
| Severe neutropenia | < 500 | /µL | High risk — act |
| Very severe / agranulocytosis | < 200 | /µL | Critical risk |
* Reference ranges may vary by laboratory and patient population. Pediatric thresholds differ from adult values and should be verified with age-specific norms. These classifications reflect widely cited international guidelines.
Head-to-Head Comparison Table
| Feature | Leukopenia | Neutropenia |
|---|---|---|
| Definition | Low total WBC count | Low absolute neutrophil count (ANC) |
| Diagnostic threshold | WBC < 4,000/µL | ANC < 1,500/µL |
| Cell types affected | All leukocyte subtypes | Neutrophils (segmented + bands) only |
| Infection risk predictor? | Indirect / partial | Direct and quantified by severity |
| Requires ANC calculation? | Yes — always | Yes — defines the condition |
| Can occur with normal WBC? | No (by definition) | Yes — neutropenia with normal WBC is possible |
| Primary diagnostic utility | Signals a need for differential analysis | Directly guides infection management strategy |
Clinical Causes and Associated Conditions
Causes of leukopenia
Infections
- Influenza and other viral illnesses
- Epstein–Barr virus (EBV/mononucleosis)
- Viral hepatitis (B and C)
- HIV (early and late disease)
- Early-phase sepsis
Bone Marrow Suppression
- Cytotoxic chemotherapy
- Radiation therapy
- Aplastic anemia
- Myelodysplastic syndrome (MDS)
Autoimmune / Systemic
- Systemic lupus erythematosus (SLE)
- Rheumatoid arthritis (Felty syndrome)
- Sjögren syndrome
Nutritional / Drug-Induced
- Vitamin B12 deficiency
- Folate deficiency
- Antithyroid agents (methimazole)
- Anticonvulsants, certain antibiotics
Causes of neutropenia
Oncology / Treatment-Related
- Chemotherapy-induced neutropenia
- Radiation therapy to marrow sites
- Post-stem-cell transplant engraftment failure
Hematologic Disorders
- Myelodysplastic syndrome (MDS)
- Aplastic anemia
- Kostmann syndrome (congenital)
- Cyclic neutropenia
Immune-Mediated
- Autoimmune neutropenia
- Drug-induced immune neutropenia
- Post-infectious immune neutropenia
Drug-Induced
- Methimazole / propylthiouracil (PTU)
- Clozapine (requires WBC monitoring)
- Sulfonamides, beta-lactam antibiotics
- NSAIDs, carbamazepine
Drug-induced agranulocytosis: Clozapine and methimazole are among the most important causes of severe drug-induced neutropenia. Patients on these agents require scheduled ANC monitoring per protocol. Sudden onset of fever or sore throat in these patients warrants urgent CBC assessment.
Precautions and Interpretation Pitfalls
Accurate interpretation of leukopenia and neutropenia requires attention to several analytical and clinical variables that can profoundly affect results:
01. Always calculate the ANC — never rely on total WBC alone. A normal WBC can coexist with significant neutropenia. Conversely, leukopenia may be entirely lymphocyte-driven with a preserved neutrophil count. The differential is mandatory.
02. WBC is highly sensitive to physiologic variables. Physical exercise, emotional stress, cigarette smoking, dehydration, and epinephrine release can transiently elevate WBC by demarginating neutrophils. Conversely, morning draws in resting patients may show physiologically lower counts.
03. Sample handling errors directly affect cell counts. Inadequate inversion of the EDTA tube causes microclot formation, which sequesters leukocytes and yields falsely low counts. All CBC tubes must be gently inverted 8–10 times immediately after venipuncture.
04. Obtain a complete medication history before ordering the test. Corticosteroids can elevate neutrophil counts by demargination and impair lymphocyte trafficking. Antithyroid agents, clozapine, and sulfonamides are direct bone marrow suppressants. Interpreting results without knowing the medication list is diagnostically unreliable.
05. Febrile neutropenia is an emergency — do not wait for cultures. A temperature of ≥38.3°C (or ≥38.0°C sustained over one hour) in a patient with ANC <500/µL requires immediate empirical broad-spectrum antibiotic therapy. Delaying treatment while awaiting laboratory results increases mortality risk substantially.
Self-diagnosis warning: A low WBC on a report does not establish any diagnosis. These results must be interpreted by a physician in the context of clinical symptoms, medication history, and the patient’s full medical background. Do not attempt to self-diagnose based on laboratory values alone.
Specialist’s Perspective and Key Takeaways
In my laboratory practice, the single most consequential interpretive error I witness is a physician concluding that a patient is “fine” because the total WBC is only slightly low, without calculating the ANC. Equally problematic is the reverse — panic over leukopenia that turns out to be benign lymphopenia in a recovering viral illness. The CBC differential is not a detail; it is the clinical substance of the result. Train yourself to reach for the ANC automatically whenever the WBC is low — or whenever your patient is febrile and immunocompromised, regardless of the WBC.
— Laboratory Medicine Specialist, MD.phD.
- Leukopenia (WBC <4,000/µL) requires differential analysis before drawing any clinical conclusions — ask which cell type is reduced.
- Neutropenia is defined by ANC <1,500/µL and is the primary determinant of bacterial and fungal infection risk.
- Always calculate ANC using: WBC × (% segs + % bands) / 100. Do not estimate from the total WBC.
- Severe neutropenia (ANC <500/µL) with fever is febrile neutropenia — initiate empirical antibiotics immediately.
- Drug history is essential: clozapine, methimazole, and sulfonamides are among the leading reversible causes of neutropenia.
- Benign ethnic neutropenia is a real entity and should be considered before pursuing invasive bone marrow evaluation in low-risk patients.
About the Author
MD.phD.
The author is a board-certified Laboratory Medicine Specialist with subspecialty training in clinical hematology, flow cytometry, and morphologic blood cell analysis. They hold academic appointments and contribute to laboratory quality improvement initiatives. Content in this article is for educational purposes and reflects current evidence-based practice guidelines.
https://medlabinsight.com/body-fluid-analysis-interpretation-guide/
https://medlabinsight.com/weak-d-test-purpose-method-interpretation/
References
- Dale, D. C. (2023). Drug-induced neutropenia and agranulocytosis. UpToDate. Retrieved from uptodate.com
- Newburger, P. E., & Dale, D. C. (2013). Evaluation and management of patients with isolated neutropenia. Seminars in Hematology, 50(3), 198–206. https://doi.org/10.1053/j.seminhematol.2013.06.010
- National Cancer Institute. (2024). Common Terminology Criteria for Adverse Events (CTCAE), v5.0. U.S. Department of Health and Human Services.
- Freifeld, A. G., Bow, E. J., Sepkowitz, K. A., et al. (2011). Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer. Clinical Infectious Diseases, 52(4), e56–e93. https://doi.org/10.1093/cid/cir073
- Hsieh, M. M., Everhart, J. E., Byrd-Holt, D. D., et al. (2007). Prevalence of neutropenia in the U.S. population. Annals of Internal Medicine, 146(7), 486–492. https://doi.org/10.7326/0003-4819-146-7-200704030-00004
- Mayo Clinic. (2024). Neutropenia: Symptoms and causes. Retrieved from mayoclinic.org
- Medscape. (2024). Leukopenia workup and treatment. Retrieved from emedicine.medscape.com