Weak D Test (Du Test): A Laboratory Medicine Specialist’s Complete Guide to Purpose, Interpretation & Transfusion Guidelines
Written by a Laboratory Medicine Specialist (MD.phD.)
Introduction
The Weak D test — sometimes historically called the Du test — is one of the most clinically consequential yet frequently misunderstood assays in transfusion medicine. As a Laboratory Medicine Specialist, I want to provide a definitive, evidence-based guide that cuts through the confusion. In brief: the Weak D test is performed when routine RhD typing yields a weak or ambiguous result, and its interpretation directly determines whether a patient receives RhD-positive or RhD-negative blood products, and whether a pregnant woman requires Rh immunoglobulin (RhIg) prophylaxis. Getting this test right matters enormously — a misclassification can lead to alloimmunization, hemolytic transfusion reactions, or hemolytic disease of the fetus and newborn (HDFN).
What Is the Weak D Test & Why Is It Ordered?
Defining Weak D
The RhD antigen is the most immunogenic red blood cell antigen after ABO. Most individuals are straightforwardly RhD-positive or RhD-negative. However, a subset of individuals carry reduced quantities of D antigen on their red cell surface — too few to trigger a clear positive reaction in standard direct agglutination typing, yet enough to be clinically significant. These individuals are classified as Weak D (formerly called Du).
Weak D arises from missense mutations in the RHD gene, resulting in a D antigen that is quantitatively diminished but qualitatively intact (in most types). This is distinct from Partial D, where the D antigen is qualitatively altered — meaning certain D epitopes are missing and the individual can produce alloanti-D if exposed to normal D-positive red cells.
Clinical Indications — When Is This Test Ordered?
A physician or blood bank specialist orders the Weak D test in the following situations:
Weak or equivocal RhD typing result — when the initial tube or gel card D typing shows a reaction of 0 to 1+, making a definitive positive or negative call impossible.
Confirming true RhD-negative status — to rule out Weak D before assigning a patient as RhD-negative, since misclassification may result in unnecessary use of scarce RhD-negative blood.
Obstetric management — determining whether a pregnant woman is truly RhD-negative or Weak D, which affects the decision to administer antenatal and postnatal RhIg.
Neonatal workup — newborns with a weak D reaction on cord blood typing require Weak D testing before finalizing the RhD type.
Blood donor screening — donors with a Weak D result are labeled and their units handled as RhD-positive to protect recipients.
Specimen Requirements
Parameter
Specification
Specimen type
EDTA whole blood (purple/lavender-top tube)
Volume
Minimum 3 mL (check local lab policy)
Storage
Refrigerated (2–8°C); test within 24–48 hours of collection
Rejection criteria
Hemolyzed, clotted, or grossly lipemic samples
⚠️ Note: EDTA anticoagulant is preferred because it preserves red cell antigen integrity and prevents complement activation that can interfere with indirect antiglobulin testing.
How Is the Test Performed? (Methodology)
The vast majority of modern blood banks perform the Weak D test using the Microcolumn Gel (ID-Card / BioVue) technique, which provides superior standardization and sensitivity compared to older tube methods.
Microcolumn Gel Indirect Antiglobulin Test (IAT) — Step by Step
Red cell preparation: A suspension of the patient’s washed red cells is prepared.
Sensitization (37°C incubation): The red cells are incubated with a licensed anti-D reagent (IgG class) at 37°C for 15 minutes. At this stage, the anti-D binds to D antigen sites on the red cell surface — even the sparse antigen sites of Weak D cells.
Gel card centrifugation: The sensitized cells are transferred into a microcolumn gel card containing anti-human globulin (AHG) — the Coombs reagent. During centrifugation, the AHG bridges IgG-coated red cells, forming a lattice.
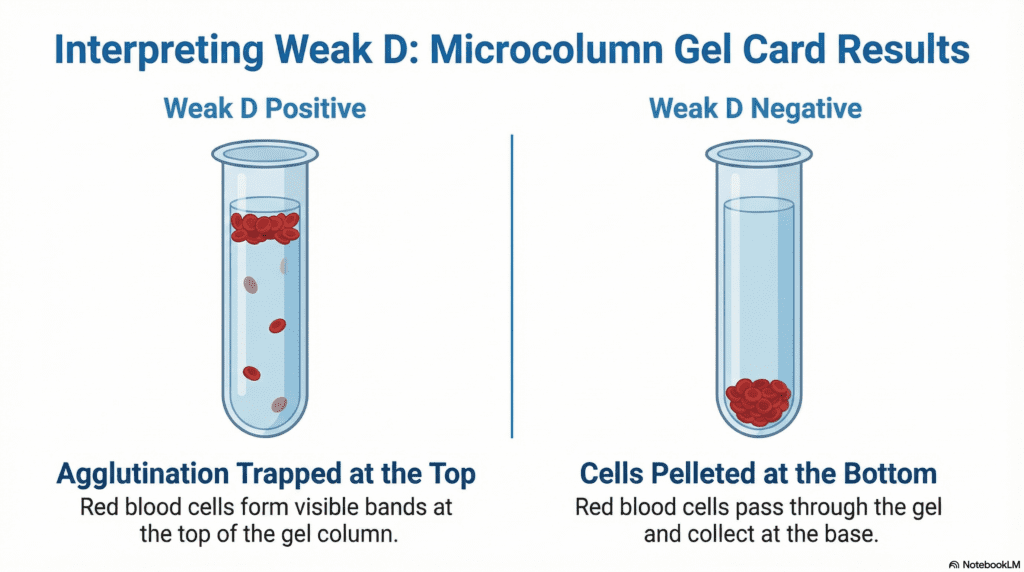
Result reading:
Positive (Weak D detected): Agglutinated cells are trapped in the upper portion of the gel column — a clear red band or diffuse agglutination.
Negative (no Weak D): Uncoated cells pass freely through the gel and pellet at the bottom of the column.
Why Use Gel Over Tube?
The traditional tube IAT required multiple wash steps to remove unbound globulin before adding AHG — a process prone to technique-dependent variation. Gel cards eliminate wash steps, reducing false negatives from inadvertent elution of weakly bound antibody, and provide a permanently readable, photographable result.
Reference Ranges & Result Interpretation
Unlike quantitative laboratory tests (e.g., serum creatinine), the Weak D test does not produce a numerical result. Interpretation is based on agglutination grading.
Result
Agglutination Pattern
Interpretation
Weak D Positive
Any agglutination in the gel column (0.5+ to 3+)
D antigen present in reduced quantity
Weak D Negative
Red cells pellet at column bottom; no agglutination
No D antigen detected — true RhD-negative
Indeterminate
Mixed-field or very faint reaction
Requires reflex RHD genotyping
⚠️ Reference ranges may vary by laboratory reagent, card lot, and reading method. Always interpret in conjunction with the full clinical picture.
Clinical Interpretation
Weak D Positive — What Does It Mean?
A positive Weak D result tells you that D antigen is present, but it does not tell you which type of Weak D the patient has. This distinction is critical.
Weak D Type 1, 2, and 3 account for approximately 90% of Weak D cases in European populations. These individuals:
Express a quantitatively reduced but qualitatively complete D antigen
Do not produce alloanti-D when exposed to RhD-positive blood
Can safely receive RhD-positive blood products
Pregnant women confirmed as Type 1, 2, or 3 by genotyping do not require RhIg (per current AABB and British Committee for Standards in Haematology guidance, though institutional policies vary)
Partial D variants (including DAR, DVI, DVII, and others) and rare Weak D types (e.g., Type 4.0, Type 4.2/DAR):
Have qualitative alterations — certain RhD epitopes are absent
Can produce alloanti-D upon exposure to normal D-positive red cells
Must be managed as RhD-negative for transfusion and obstetric purposes
Weak D Negative — What Does It Mean?
A negative Weak D test, following a negative direct D typing, confirms the patient is truly RhD-negative. These patients should receive RhD-negative blood and, if pregnant, are candidates for RhIg prophylaxis per standard protocols.
Transfusion & Obstetric Guidelines
For Adult Patients Requiring Transfusion
Patient’s Weak D Status
Recommended Blood Product
Notes
Weak D Type 1, 2, or 3 (confirmed by genotype)
RhD-positive acceptable
RhD-negative is always safer if available
Partial D or unknown Weak D type
RhD-negative required
Prevent alloimmunization
Weak D type unknown, urgent transfusion
RhD-negative preferred
Conservative approach until typing complete
For Pregnant Women
A pregnant patient with a Weak D result should undergo RHD genotyping where available.
If confirmed as Type 1, 2, or 3: RhIg may be withheld (per ACOG/AABB updated guidance) — though many institutions still administer it pending local policy.
If Partial D or type unknown: administer RhIg as for a standard RhD-negative patient.
RhIg prevents maternal sensitization that could cause HDFN in future pregnancies.
For Neonates
Cord blood with a weak D reaction → perform Weak D test before finalizing the report.
If the neonate is Weak D positive (any type): label as RhD-positive; if the mother is RhD-negative, evaluate whether maternal anti-D is present (direct antiglobulin test on cord blood).
Precautions & Limitations
Several factors can confound Weak D test results, and every laboratorian should be aware of them:
False Negative Results
Improper incubation temperature or shortened incubation time
Failure to use an IgG-class anti-D reagent (IgM reagents will not sensitize cells for AHG detection)
Hemolyzed or aged specimens with degraded antigen
Rare cases of antigen masking in leukemia or other hematologic conditions
False Positive Results
Polyagglutination (T-activation, Tn activation) in certain bacterial infections
Rouleaux formation in hyperglobulinemia
Contaminated reagents or equipment
Inherent Limitation: Cannot Distinguish Weak D Types The gel IAT Weak D test cannot differentiate Type 1/2/3 from Partial D. This is the single most important limitation. When the clinical stakes are high — pregnant women, multiply transfused patients, or any patient with a previous anti-D — RHD genotyping is the definitive answer.
A single Weak D test result must never be used for self-diagnosis or independent clinical decision-making. Always interpret in the context of the full clinical history, ABO/Rh phenotype, antibody screen, and genotype data where available.
Specialist’s Perspective & Conclusion
In my experience in laboratory medicine, the Weak D test is a textbook example of a test where the result is only the beginning of the interpretation — not the end. When I receive a Weak D-positive result on a pregnant patient, my immediate next question is always: what type? The difference between a Type 1 and a Partial D (such as DVI) is the difference between reassuring a patient she doesn’t need an injection and ensuring she absolutely does.
My practical recommendations:
Routinely offer RHD genotyping for all obstetric patients with a Weak D result — it eliminates ambiguity and can spare patients from unnecessary RhIg injections.
Default to conservative management (treat as RhD-negative) whenever genotyping is unavailable or results are pending.
Educate clinical teams that “Weak D positive” does not automatically mean the patient is RhD-positive for all purposes — the nuance matters enormously.
Never skip the Weak D test in neonates with ambiguous D typing — HDFN management depends on it.
The Weak D test, when properly performed and interpreted alongside molecular typing, is an indispensable tool in safe transfusion practice and maternal-fetal medicine.
Author Profile
This article was written by a board-certified Laboratory Medicine Specialist (MD) with expertise in transfusion medicine, immunohematology, and clinical pathology. The author has extensive experience in blood bank operations, RhD variant management, and obstetric hematology consultation at a university-affiliated medical center.
Denomme, G. A., Dake, L. R., Vilensky, D., Ramyar, L., & Judd, W. J. (2008). Rh discrepancies caused by variable reactivity of partial and weak D types with different serologic techniques. Transfusion, 48(3), 473–478. https://doi.org/10.1111/j.1537-2995.2007.01559.x
Sandler, S. G., Flegel, W. A., Westhoff, C. M., Denomme, G. A., Eder, A. F., Redman, M., & Sipherd, B. D. (2015). It’s time to phase in RHD genotyping for patients with a serologic weak D phenotype. Transfusion, 55(3), 680–689. https://doi.org/10.1111/trf.12941
American College of Obstetricians and Gynecologists (ACOG). (2017). Prevention of Rh D Alloimmunization: Practice Bulletin No. 181. ACOG. https://www.acog.org
AABB Technical Manual, 20th Edition. (2020). American Association of Blood Banks. Bethesda, MD: AABB Press.
Fung, M. K., Grossman, B. J., Hillyer, C. D., & Westhoff, C. M. (Eds.). (2014). AABB Technical Manual (18th ed.). AABB.
Garratty, G. (2008). Immunohematology problems associated with determining RhD type. Laboratory Medicine, 39(8), 472–477.
🩸 Understanding MCV, MCH, MCHC, RDW, MPV, PCT, and PDW in CBC A Complete Guide to RBC and Platelet Indices Complete Blood Count (CBC) is one of the most fundamental yet clinically powerful laboratory tests.Beyond simple cell counts, RBC indices (MCV, MCH, MCHC, RDW) and platelet indices (MPV, PCT, PDW) provide key diagnostic insights into…
Why White Blood Cells Can Drop During Infection: A Specialist’s Guide to Leukocyte Margination and WBC Distribution Written by a Laboratory Medicine Specialist (MD) Introduction As a Laboratory Medicine Specialist, few findings generate more urgent phone calls from clinical colleagues than an unexpectedly low white blood cell count in a patient who is clearly unwell….
🧪 LAP Score (Leukocyte Alkaline Phosphatase): Complete Guide CML vs. Leukemoid Reaction · Staining · Reference Range · Interpretation 1. What Is the LAP Score? (Definition) The Leukocyte Alkaline Phosphatase (LAP) score is a cytochemical test that measures the activity of alkaline phosphatase in neutrophils and their precursors. Historically essential for distinguishing Chronic Myeloid Leukemia…
🧬 ADAMTS13 Activity Test — Complete Guide Key diagnostic test for thrombotic thrombocytopenic purpura (TTP)Principle · ELISA method · Reference range · Clinical significance · Interpretation points Professional guide to ADAMTS13 Activity by a medical specialist 1. What Is ADAMTS13? ADAMTS13 (A Disintegrin And Metalloprotease with ThromboSpondin type 1 motif, 13) is a plasma metalloprotease…
🩸 Complete Blood Count (CBC) Basics WBC · RBC · Hb · Hct · Platelet — Clinical Meaning & Interpretation Guide A Complete Blood Count (CBC) measures white blood cells (WBC), red blood cells (RBC), hemoglobin (Hb), hematocrit (Hct), and platelets (PLT).It is one of the most essential laboratory tests used to evaluate infection, inflammation,…
🦟 Filaria (Microfilaria) Test — Complete Diagnostic Guide Transmission · Test Purpose · Microscopy Features · Stain Methods · Interpretation Notes Filarial worms are parasitic nematodes transmitted primarily through mosquitoes, capable of infecting lymphatic vessels, subcutaneous tissue, nodules, and the eyes. Several species cause significant human disease worldwide. Major filarial species include: 1. What Is…