What is Serum Amyloid A (SAA) Test?
Understanding Serum Amyloid A (SAA): A Specialist’s Guide to This Rapid Inflammatory Marker
As a specialist in Laboratory Medicine, I closely monitor biomarkers that allow for the earliest possible detection of disease. While C-Reactive Protein (CRP) is the household name for inflammation, Serum Amyloid A (SAA) is often the “hidden gem” of the clinical lab. SAA is an acute-phase protein that increases significantly—sometimes by 1,000-fold—within hours of infection or tissue injury. This guide explores why SAA is becoming a critical tool for diagnosing acute infections, monitoring chronic autoimmune diseases, and predicting the risk of secondary amyloidosis.
What is the Serum Amyloid A (SAA) Test & Its Purpose
Serum Amyloid A (SAA) refers to a family of apolipoproteins associated with high-density lipoprotein (HDL) in the plasma. Synthesized primarily in the liver, its production is stimulated by pro-inflammatory cytokines like IL-1, IL-6, and TNF-α.
In clinical practice, a Laboratory Medicine Specialist orders an SAA test for several key reasons:
- Early Detection of Acute Inflammation: SAA levels rise faster and more significantly than CRP, often within 4–6 hours of an insult.
- Differentiating Viral vs. Bacterial Infections: Unlike CRP, which may remain low during certain viral infections, SAA tends to rise in both, making it a highly sensitive (though non-specific) marker.
- Monitoring Chronic Disease Activity: It is used to track the “smoldering” inflammation in conditions like Rheumatoid Arthritis (RA) or Inflammatory Bowel Disease (IBD).
- Assessing Risk of AA Amyloidosis: Chronic elevation of SAA can lead to protein deposits in organs (kidneys, heart, GI tract), leading to organ failure.
Measurement Principle: Latex Immunoturbidimetry
In modern automated laboratories (such as those using Roche cobas® systems), SAA is measured using Latex Immunoturbidimetry. Latex particles coated with anti-SAA antibodies react with the SAA in the patient’s serum, creating immune complexes that increase the turbidity of the solution. The analyzer measures this light scattering to provide a precise concentration within minutes.
Normal Reference Ranges
While specific “normal” values can fluctuate based on the manufacturer of the assay (e.g., Siemens, Roche, or Abbott), the following is the generally accepted clinical standard.
| Category | Normal Range | Unit |
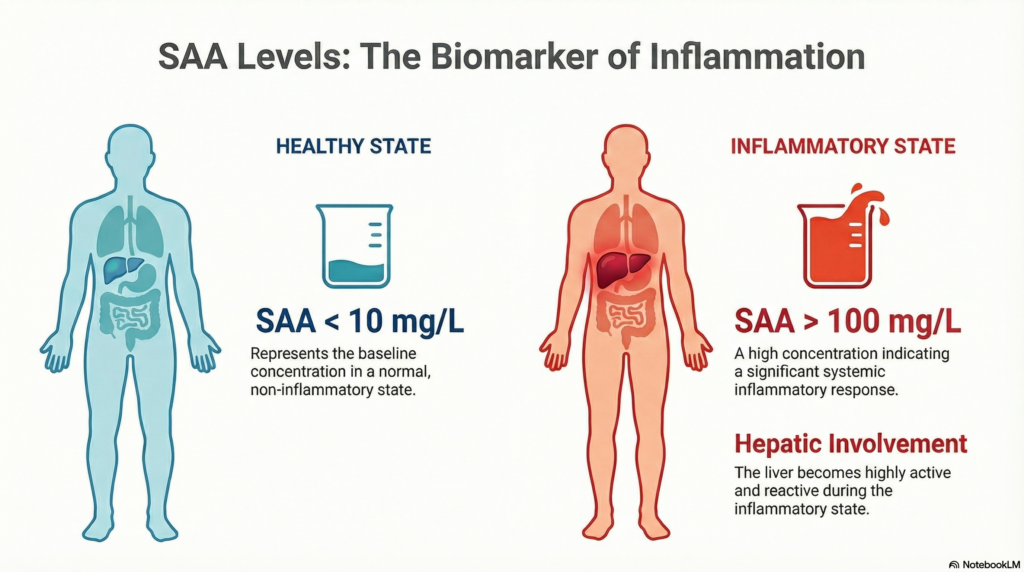
| Healthy Adults | < 10.0 | mg/L |
| Minor Inflammation | 10.0 – 50.0 | mg/L |
| Acute Infection/Injury | > 100.0 | mg/L |
Note: Reference ranges may vary by laboratory. Always consult the specific reference interval provided on your lab report.
Clinical Interpretation
High Levels (Increased SAA)
A high SAA level is a “red flag” for systemic inflammation. Because SAA has a very short half-life, a high value indicates an active, ongoing process.
- Infections: Acute bacterial sepsis, pneumonia, and viral infections (including COVID-19 and Influenza).
- Autoimmune Disorders: Active flares of Rheumatoid Arthritis (RA), Ankylosing Spondylitis (AS), and Psoriatic Arthritis.
- Gastrointestinal Disease: Crohn’s disease and Ulcerative Colitis.
- Tissue Damage: Major surgery, myocardial infarction (heart attack), or severe trauma/burns.
- Malignancy: Certain cancers, particularly renal cell carcinoma and lung cancer, can trigger an SAA response.
Low Levels (Decreased SAA)
Since SAA is normally near-zero in healthy individuals, “low” levels are generally expected. However, an inappropriately low level during a known infection might indicate:
- Severe Liver Dysfunction: As the liver is the primary site of SAA synthesis, end-stage liver disease can blunt the acute-phase response.
- Immunosuppression: Use of certain biologics or high-dose steroids that inhibit cytokine signaling.
Precautions & Limitations
While SAA is incredibly sensitive, it is important to remember its limitations:
- Non-Specificity: A high SAA tells us that there is inflammation, but it does not tell us where or why. It must be interpreted alongside clinical symptoms and imaging.
- Biological Variation: Factors like obesity or pregnancy can slightly elevate baseline SAA levels due to low-grade systemic stress.
- Glucocorticoids: Patients on steroid therapy may show suppressed SAA levels even in the presence of an infection.
Specialist’s Perspective & Conclusion
In my experience as a Laboratory Medicine Specialist, the true value of SAA lies in its kinetics. Because SAA drops rapidly once the inflammatory stimulus is removed, it is an excellent tool for “therapeutic monitoring.” If we start a patient on antibiotics for sepsis and the SAA drops by 50% within 24 hours, we know the treatment is working—often before the patient’s fever even breaks.
Key Takeaway: SAA is a high-sensitivity “radar” for inflammation. If your SAA is elevated, it warrants a deep dive into potential infectious or autoimmune triggers to prevent long-term complications like amyloidosis.
Author Profile: MD, Laboratory Medicine Specialist
The author is a board-certified Laboratory Medicine Specialist (MD, PhD) specializing in clinical pathology and biomarker kinetics. With over 15 years of experience in diagnostic medicine, they focus on integrating advanced laboratory data into actionable clinical insights for better patient outcomes.
HCV RNA PCR Test: A Laboratory Specialist’s Complete Guide – MedLab Insight
References
- UpToDate. (2024). Acute phase reactants. * Mayo Clinic Laboratories. Serum Amyloid A Clinical Utility and Methodology.
- Sack, G. H. (2018). Serum Amyloid A – A Review. Molecular Medicine, 24(1), 46.
- Medscape. AA Amyloidosis: Practice Essentials, Pathophysiology, and Etiology.