
[MD.PhD.] Urinary Urea Nitrogen (UUN) (26)
Understanding Urinary Urea Nitrogen (UUN): A Laboratory Medicine Specialist’s Guide to Clinical Interpretation
Written by a Board-Certified Laboratory Medicine Specialist (MD.PhD.), this comprehensive guide explains what the UUN test measures, why it matters in clinical practice, and how to correctly interpret elevated or decreased results in various patient scenarios.
Quick summary: The Urinary Urea Nitrogen (UUN) test measures the amount of nitrogen excreted in the form of urea in a 24-hour urine collection. It is a cornerstone tool for assessing protein catabolism, monitoring nutritional support, and evaluating nitrogen balance in critically ill patients. Abnormal results may indicate high-protein intake, catabolic states such as sepsis or trauma, liver failure, kidney disease, or protein malnutrition.
What is the UUN test & why is it ordered?
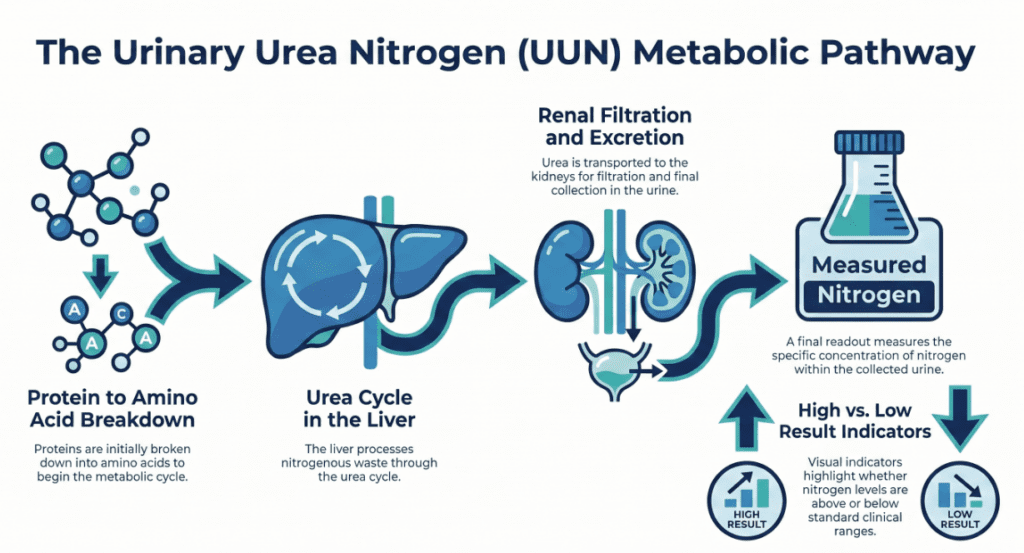
Urea is the primary end-product of protein metabolism in the human body. When proteins are broken down, amino acids are deaminated and the resulting ammonia is converted to urea via the hepatic urea cycle. This urea is subsequently filtered and excreted by the kidneys. The Urinary Urea Nitrogen (UUN) test quantifies only the nitrogen fraction of excreted urea — providing a reliable, quantitative window into whole-body protein turnover.
Clinicians order the UUN test for several key reasons:
- Protein catabolic rate assessment: Quantifying the degree of muscle and protein breakdown in surgical, trauma, or septic patients.
- Nutritional monitoring: Determining whether parenteral (TPN) or enteral (EN) nutrition is providing adequate protein to meet metabolic demands.
- Nitrogen balance calculation: Guiding protein prescription in the ICU — a critical tool in preventing protein-energy malnutrition.
- Indirect renal function evaluation: Detecting changes in urea excretion that may reflect kidney dysfunction.
- Protein intake verification: Correlating measured dietary protein against actual metabolic output.
Clinical note: The nitrogen balance equation is: Nitrogen Balance = Protein Intake (g/day) ÷ 6.25 − (UUN + 4 g for non-urea nitrogen losses). A negative balance indicates net protein catabolism.
Specimen, methodology & measurement principle
The gold-standard specimen is a 24-hour urine collection. Random (spot) urine may be used in some clinical contexts, but it carries significantly lower accuracy for protein metabolism assessment and is not recommended for formal nitrogen balance calculations.
The laboratory measures UUN using the Urease–GLDH (Glutamate Dehydrogenase) coupled enzymatic method, the current international standard on automated chemistry analyzers:
- Step 1 — Urease reaction: Urease enzyme hydrolyzes urea in the urine sample to ammonium (NH₄⁺) and carbon dioxide.
- Step 2 — GLDH reaction: Ammonium participates in the GLDH-catalyzed reaction, oxidizing NADH to NAD⁺.
- Step 3 — Photometric detection: The decrease in absorbance at 340 nm is measured and is directly proportional to urea concentration, from which the nitrogen content is mathematically derived.
This method offers high precision, linearity, and excellent suitability for high-throughput laboratory automation.
Normal reference ranges
| Category | Normal range | Unit / notes |
|---|---|---|
| Adults (24-hour urine) | 6,500 – 13,000 | mg/day |
| High-protein diet | May exceed 13,000 | mg/day (expected physiological rise) |
| Low-protein / fasting state | May fall below 6,500 | mg/day (expected physiological decrease) |
| Critical care / catabolic state | Often >15,000 – 20,000+ | mg/day; indicates severe hypercatabolism |
* Reference ranges may vary by laboratory and are strongly influenced by dietary protein intake. Always interpret in the context of the patient’s nutritional status.
Clinical interpretation
Elevated UUN — causes & mechanisms
- High-protein dietary intake: The most common physiological cause. Excess amino acids are catabolized and nitrogen is excreted as urea.
- Sepsis / severe infection: Systemic inflammation activates catecholamines and cortisol, driving accelerated muscle proteolysis and greatly increased urea production.
- Major surgery & trauma: The post-operative catabolic stress response causes significant protein breakdown, often resulting in UUN values of 15–25 g/day.
- Burns: One of the most hypercatabolic states known — protein losses through wound exudate and increased metabolic demands can push UUN to extreme levels.
- Cancer cachexia: Chronic systemic inflammation and tumor-derived factors promote relentless muscle wasting.
- Hyperthyroidism: Excess thyroid hormones accelerate protein turnover, increasing urea generation and excretion.
- High-protein TPN/EN: Deliberate delivery of protein in excess of metabolic requirements leads to increased urea nitrogen excretion.
Decreased UUN — causes & mechanisms
- Protein malnutrition / starvation: Reduced amino acid substrate for urea synthesis results in diminished UUN.
- Severe hepatic failure: The urea cycle is located in the liver. When hepatic synthetic function collapses, urea formation drops precipitously — UUN falls despite ongoing muscle proteolysis. This is a critical interpretive pitfall.
- Severe chronic kidney disease / end-stage renal disease: Markedly reduced GFR limits urea filtration and excretion, resulting in low urinary UUN even when blood urea nitrogen (BUN) is elevated.
- Anabolic recovery states: During healing and rehabilitation, nitrogen is retained for tissue synthesis, reducing urinary excretion.
Precautions & limitations
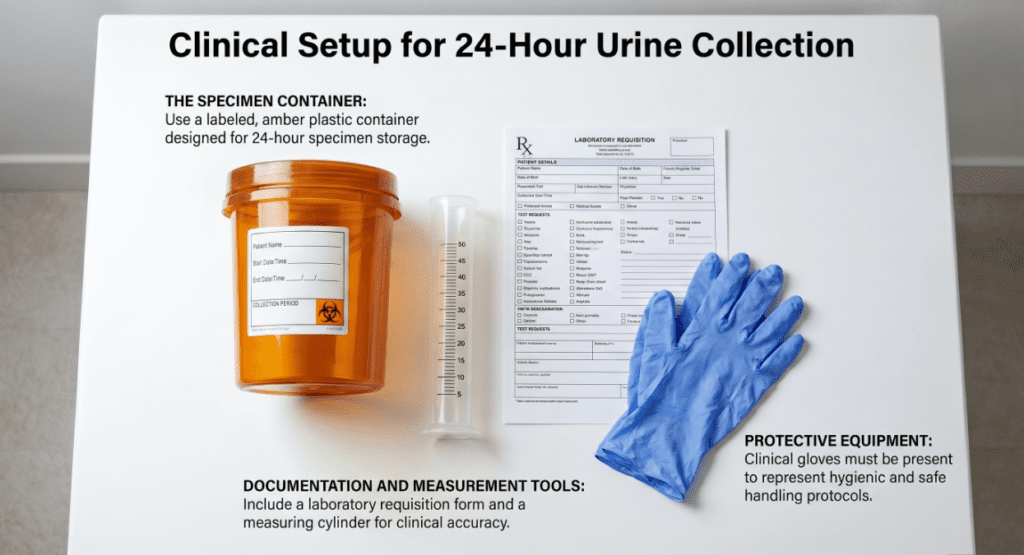
- 24-hour collection accuracy is paramount. Incomplete collections (missed voids, incorrect storage) are the single largest source of error. Patients and nursing staff require clear collection instructions.
- Interpret alongside protein intake. UUN in isolation provides an incomplete picture; it must always be cross-referenced with the patient’s actual protein intake to calculate nitrogen balance.
- Non-urea urinary nitrogen (NUUN) accounts for 15–20% of total nitrogen loss. This includes creatinine, ammonia, uric acid, and other nitrogen-containing compounds. When precision is required — particularly in burn patients or those with complex metabolic disorders — Total Urinary Nitrogen (TUN) measurement is preferable.
- Liver failure creates a diagnostic trap. UUN may appear falsely low or normal in severe hepatic failure because the urea cycle is impaired, even when actual protein catabolism is severe. Clinicians must not be falsely reassured by a “normal” UUN in a cirrhotic patient with muscle wasting.
- Renal failure distorts excretion. In patients with significantly reduced GFR, urinary UUN underestimates true protein catabolism; BUN accumulates in the blood rather than being excreted in urine.
- Medications: Corticosteroids increase protein catabolism and raise UUN; anabolic hormones may reduce it.
- This test should not be used for self-diagnosis. Interpretation requires integration with clinical findings, dietary records, metabolic status, and other laboratory data by a qualified physician.
Summary reference table
| Parameter | Details |
|---|---|
| Test name | Urinary Urea Nitrogen (UUN) |
| Specimen | 24-hour urine (preferred); random urine acceptable for screening only |
| Method | Urease–GLDH enzymatic photometric assay (340 nm) |
| Reference range | 6,500 – 13,000 mg/day (adult, normal diet) |
| Elevated | High-protein intake, sepsis, trauma, burns, hyperthyroidism, TPN excess |
| Decreased | Protein malnutrition, severe liver failure, advanced renal failure |
| Key limitation | Must be interpreted with protein intake and clinical context; liver/kidney disease distort results |
Specialist’s perspective & conclusion
In my clinical experience, the UUN test is among the most underutilized yet profoundly informative tests available in the nutrition assessment toolkit. In the ICU setting, it is invaluable — a patient admitted with septic shock who shows a UUN of 20 g/day is losing approximately 125 g of protein per day. Without this measurement, clinicians may be providing inadequate protein support without knowing it.
The greatest interpretive hazard I encounter is misreading a “low-normal” UUN in a patient with decompensated cirrhosis as reassuring. Liver failure suppresses urea synthesis, masking the true — and often catastrophic — degree of protein wasting occurring at the muscular level. In such cases, combining UUN with serum albumin trends, prealbumin, and clinical muscle mass assessment (CT-based sarcopenia scoring where available) gives a far more accurate metabolic picture.
Key takeaway: UUN is not just a number — it is a real-time metabolic signal. Used correctly alongside protein intake data and patient context, it transforms nutritional management from guesswork into precision medicine.
Written by a Board-Certified Laboratory Medicine Specialist
Specialist in Laboratory Medicine & Clinical Pathology. Areas of expertise include clinical chemistry, nutritional biochemistry, and critical care laboratory diagnostics. This content is intended for educational purposes and does not constitute personal medical advice.
[MD.PhD.] High-Sensitivity Troponin T (hs-TnT) Test (26) – MedLab Insight
[MD.PhD.] Understanding Bilirubin? (26) – MedLab Insight
Some images are generated by AI.
References
- Bistrian, B. R., & Driscoll, D. F. (2023). Nutritional assessment in adults. UpToDate. Wolters Kluwer.
- Martindale, R. G., McClave, S. A., et al. (2009). Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient. Critical Care Medicine, 37(5), 1757–1761.
- National Institutes of Health, National Library of Medicine. (2024). Urea nitrogen urine test. MedlinePlus. https://medlineplus.gov
- Mitch, W. E., & Ikizler, T. A. (2010). Handbook of Nutrition and the Kidney (6th ed.). Lippincott Williams & Wilkins.
- Tietz, N. W. (Ed.). (2012). Tietz Textbook of Clinical Chemistry and Molecular Diagnostics (5th ed.). Elsevier Saunders. [Urease-GLDH methodology, Chapter 25.]
- Wesson, D. E. (2022). Assessment of renal tubular function: Urine urea nitrogen. UpToDate. Wolters Kluwer.
- Nutritional issues in older adults – UpToDate