
[MD.phD.] CRP vs. hs-CRP
CRP vs. hs-CRP: A Laboratory Medicine Specialist’s Guide to Understanding the Difference
Written by a Laboratory Medicine Specialist, MD.phD.
Introduction
As a Laboratory Medicine Specialist, one of the most common questions I receive from clinicians and patients alike is: “What is the difference between CRP and hs-CRP — aren’t they the same thing?” They measure the same protein, yes, but they ask fundamentally different clinical questions. CRP (C-reactive protein) is designed to detect significant, active inflammation or infection, while hs-CRP (high-sensitivity CRP) is engineered to measure subtle, chronic low-grade inflammation that predicts long-term cardiovascular risk. Understanding which test is ordered — and why — transforms a blood result from a number into actionable clinical insight.
What Are CRP and hs-CRP?
C-reactive protein is an acute-phase reactant synthesized by the liver in response to tissue injury, infection, or systemic inflammation. It is one of the most reliable and rapidly responding biomarkers of acute inflammatory states available in routine clinical practice.
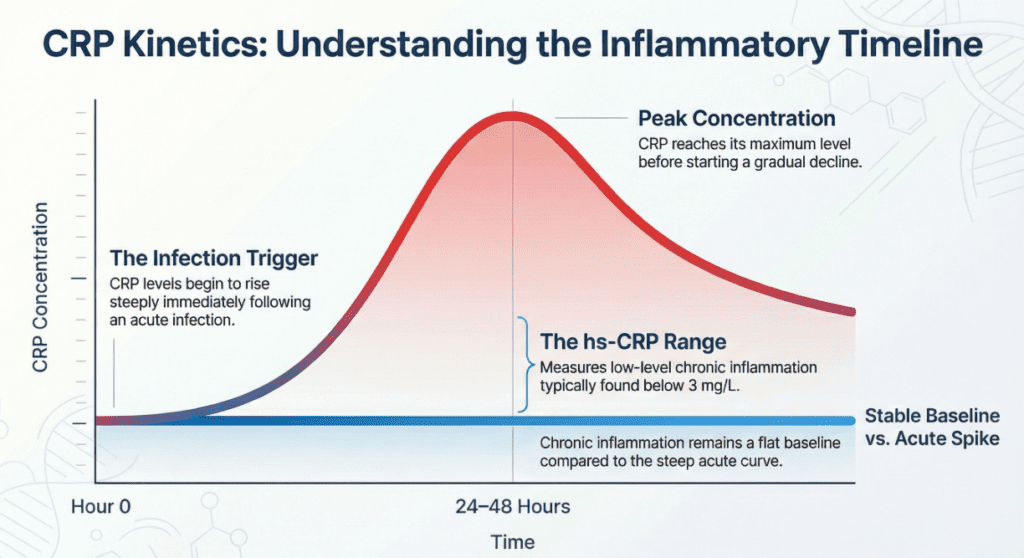
- It rises within 6–8 hours of an inflammatory trigger
- It peaks at 24–48 hours
- It has a half-life of approximately 19 hours, making it useful for monitoring the trajectory of an acute illness
Standard CRP assays are calibrated for moderate-to-high concentration ranges, making them ideal for detecting clinically obvious inflammation. They are not sensitive enough to detect the subtle, smoldering inflammation that occurs in the absence of overt illness.
hs-CRP measures the exact same protein but uses a high-sensitivity immunoassay platform capable of detecting concentrations as low as 0.1 mg/L — roughly 5 to 10 times lower than conventional CRP assays can reliably measure. This precision allows hs-CRP to characterize low-grade chronic inflammation in patients who appear entirely well — a state increasingly recognized as a driver of atherosclerosis and cardiovascular disease.
Assay Methods
The technical distinction between CRP and hs-CRP lies entirely in assay design, not in what is being detected.
Standard CRP uses latex agglutination, immunoturbidimetric assay, or nephelometry — methods optimized for speed and adequate sensitivity in high-concentration ranges typical of acute illness.
hs-CRP uses high-sensitivity immunoturbidimetric assay, enhanced nephelometry, or chemiluminescent immunoassay — methods that sacrifice some throughput for dramatically improved precision at low signal levels. The result is a measurement range of approximately 0.1 to 10 mg/L, which is precisely the range relevant to cardiovascular risk stratification in asymptomatic individuals.
Normal Reference Ranges
The interactive reference widget above provides a detailed breakdown. The key values are summarized below.
Standard CRP:
| Category | Value | Unit | Interpretation |
|---|---|---|---|
| Healthy adult | < 0.5 | mg/dL | Normal |
| Mild inflammation | 0.5 – 1.0 | mg/dL | Monitor |
| Active infection / inflammation | > 1.0 | mg/dL | Investigate |
| Severe sepsis / systemic disease | 10–40+ | mg/dL | Urgent |
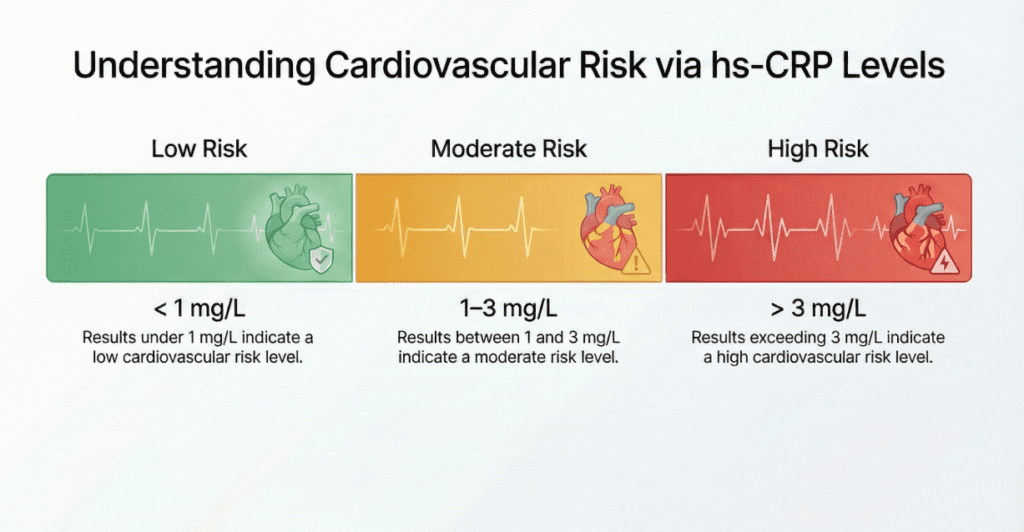
hs-CRP (cardiovascular risk tiers, per AHA/ACC guidance):
| hs-CRP Level | Unit | Cardiovascular Risk |
|---|---|---|
| < 1.0 | mg/L | Low risk |
| 1.0 – 3.0 | mg/L | Moderate risk |
| > 3.0 | mg/L | High risk |
| > 10 | mg/L | Acute process — retest after recovery |
Reference ranges may vary by laboratory platform and method.
Clinical Interpretation
Elevated CRP (increased)
A significantly elevated standard CRP — often rising to multiples of the upper reference limit — is most commonly associated with:
- Acute bacterial infections (pneumonia, urinary tract infection, cellulitis)
- Sepsis and systemic inflammatory response syndrome (SIRS)
- Active autoimmune disease flares (rheumatoid arthritis, lupus, inflammatory bowel disease)
- Post-operative or post-traumatic inflammatory response
- Solid organ rejection after transplantation
The magnitude of rise can provide directional guidance: bacterial infections typically produce higher CRP elevations than viral infections, and levels above 10 mg/dL are a strong prompt to consider a serious bacterial cause. CRP is not diagnostic in isolation, but serial measurements are extremely useful for tracking treatment response — a falling CRP generally confirms a favorable clinical trajectory.
Elevated hs-CRP (cardiovascular risk context)
An hs-CRP above 3.0 mg/L, measured in a clinically stable patient without active infection or recent illness, is associated with:
- Increased risk of myocardial infarction and stroke
- Subclinical atherosclerosis and endothelial dysfunction
- Metabolic syndrome and insulin resistance
- Obesity-associated chronic inflammation
- Increased all-cause cardiovascular mortality in long-term follow-up studies
The mechanism involves low-grade, persistent activation of the innate immune system promoting vascular inflammation and accelerating plaque development. hs-CRP is currently one of the most validated inflammatory biomarkers for cardiovascular risk prediction beyond traditional lipid-based risk calculators.
Low levels
Neither a low CRP nor a low hs-CRP is clinically concerning in isolation. However, a very low CRP in the setting of clear clinical infection may occasionally reflect impaired acute-phase response, as can be seen in severe immunosuppression or advanced liver disease. This finding should be interpreted alongside other markers such as procalcitonin, ferritin, and white cell count.
Precautions and Limitations
Several important caveats apply to both tests:
These tests cannot substitute for each other. A normal standard CRP does not make hs-CRP irrelevant. hs-CRP operates in a concentration range below the CRP assay’s reliable detection threshold. The inverse is equally true: hs-CRP is not an appropriate acute infection marker.
hs-CRP must be measured in a stable state. Any intercurrent illness — a common cold, a minor injury, vaccination within the past two weeks, recent surgery — will transiently elevate hs-CRP and invalidate its cardiovascular risk interpretation. Current guidelines recommend confirming an elevated hs-CRP result with a repeat measurement at least two weeks after full clinical recovery. If either result exceeds 10 mg/L, the acute process has not resolved and cardiovascular risk assessment is premature.
Neither test diagnoses a specific disease. CRP is a non-specific acute-phase marker. hs-CRP is a risk factor marker — not a diagnostic test for myocardial infarction or atherosclerosis. Isolated hs-CRP elevation must always be interpreted alongside fasting lipids, blood pressure, HbA1c, smoking status, and family history.
Interfering conditions. Pregnancy, obesity, oral contraceptive use, and chronic inflammatory conditions (including rheumatoid arthritis, psoriasis, and inflammatory bowel disease) can chronically elevate hs-CRP in ways that confound cardiovascular risk interpretation. Statins reliably reduce hs-CRP independently of their lipid-lowering effect — a relevant consideration when monitoring treatment response.
Single values are insufficient. Trending CRP over time during acute illness, or confirming hs-CRP stability across two measurements, provides far more clinical value than a single data point.
A Specialist’s Perspective
In the laboratory, the single most common interpretive error I see is a clinician or patient assuming that a “normal” standard CRP result means that hs-CRP is also unremarkable — or, conversely, that an elevated hs-CRP implies active infection. These tests coexist in the reference range of approximately 0.5–3 mg/dL where the two assay systems overlap, but they are designed for entirely different patient populations and clinical questions.
My practical advice: think of CRP as the “smoke detector” — it alerts you when something is actively on fire. hs-CRP is more like a carbon monoxide sensor — it quietly monitors an invisible, chronic risk that causes damage long before symptoms appear. Both are valuable. Neither replaces the other.
The most clinically powerful use of hs-CRP today is in patients with intermediate cardiovascular risk by traditional scoring (e.g., 7.5–20% ten-year ASCVD risk), where an elevated hs-CRP can tip the decision toward initiating or intensifying statin therapy — a strategy supported by the landmark JUPITER trial.
The key takeaway: read the test name on your results carefully. CRP and hs-CRP are not interchangeable labels — they represent distinct clinical strategies for answering distinct biological questions.
Author Profile
This article was authored by a board-certified specialist in Laboratory Medicine and Clinical Pathology with clinical expertise in hematology, immunochemistry, and laboratory result interpretation. All content is intended for educational purposes and does not constitute individualized medical advice. Please consult your physician or specialist for interpretation of your personal test results.
What is Serum Amyloid A (SAA) Test? – MedLab Insight
Some images in this post were generated using AI.
References
- Ridker, P. M. (2003). Clinical application of C-reactive protein for cardiovascular disease detection and prevention. Circulation, 107(3), 363–369. https://doi.org/10.1161/01.CIR.0000053730.47739.3C
- Pearson, T. A., et al. (2003). Markers of inflammation and cardiovascular disease: Application to clinical and public health practice. Circulation, 107(3), 499–511. https://doi.org/10.1161/01.CIR.0000052939.59093.45
- Ridker, P. M., et al. (2008). Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein (JUPITER trial). New England Journal of Medicine, 359(21), 2195–2207. https://doi.org/10.1056/NEJMoa0807646
- Kushner, I., & Rzewnicki, D. (2022). C-reactive protein: Clinical use. In UpToDate. Retrieved from https://www.uptodate.com
- Mayo Clinic Laboratories. (2024). C-reactive protein, high sensitivity (hs-CRP). https://www.mayocliniclabs.com
- American Heart Association / American College of Cardiology. (2019). Guideline on the primary prevention of cardiovascular disease. https://www.ahajournals.org