
[MD.PhD.] Understanding Bilirubin? (26)
Understanding Bilirubin Tests (Total, Direct & Indirect): A Laboratory Medicine Specialist’s Complete Guide
Introduction
This article is written by a Laboratory Medicine Specialist (MD.PhD.) to provide clinically accurate, evidence-based information on bilirubin testing.
Bilirubin testing is one of the most fundamental panels in laboratory medicine, ordered daily in virtually every clinical setting — from emergency departments evaluating jaundiced patients to neonatal wards monitoring newborns at risk for kernicterus. By measuring Total, Direct (conjugated), and Indirect (unconjugated) bilirubin together, clinicians can systematically narrow down the cause of jaundice, assess liver and biliary function, and detect hemolytic processes — all from a single blood draw.
In brief: Elevated total bilirubin causes jaundice. Whether the rise is driven by unconjugated (indirect) or conjugated (direct) bilirubin tells you where in the metabolic pathway the problem lies — before the liver, within it, or downstream in the bile ducts. This guide walks through the physiology, measurement methods, reference ranges, clinical interpretation, and key pitfalls every clinician and informed patient should know.
What Is the Bilirubin Test and Why Is It Ordered?
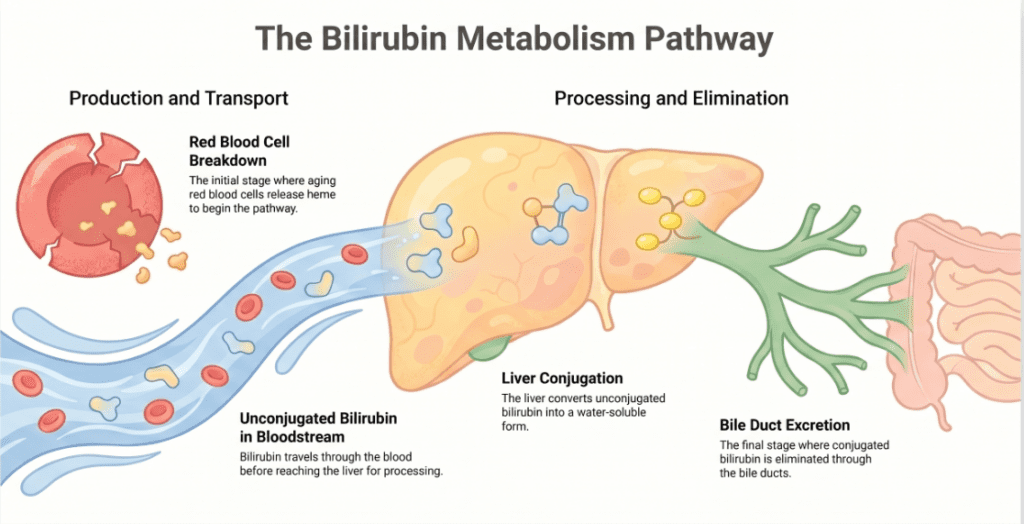
Bilirubin is a yellow-orange pigment produced when the body breaks down heme from aging red blood cells (RBCs). This breakdown occurs mainly in macrophages of the spleen, liver, and bone marrow. The resulting bilirubin is initially unconjugated (fat-soluble) and must be transported to the liver bound to albumin. There, hepatocytes conjugate it with glucuronic acid (via the enzyme UGT1A1), making it water-soluble (conjugated) and ready for excretion into bile.
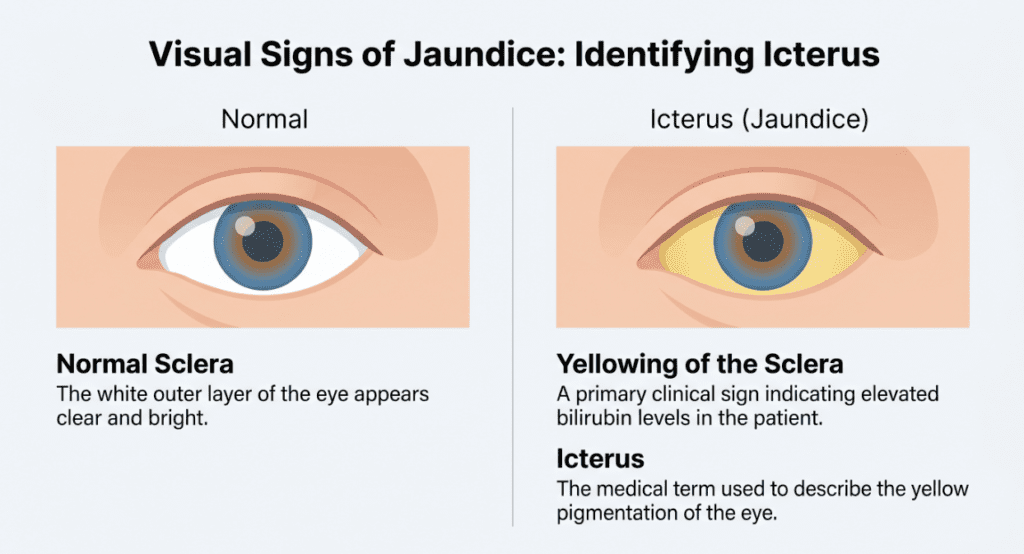
When any step in this chain fails — excessive RBC destruction, impaired hepatic uptake or conjugation, or blocked biliary drainage — bilirubin accumulates in the blood, eventually depositing in the skin and sclera, producing the clinical sign we call jaundice (icterus), typically visible when total bilirubin exceeds approximately 2.5–3.0 mg/dL.
Clinical indications for ordering bilirubin testing:
- Jaundice workup — the most common indication; differentiating pre-hepatic, hepatic, and post-hepatic causes
- Liver disease evaluation — acute/chronic hepatitis, cirrhosis, alcoholic or drug-induced liver injury
- Biliary tract assessment — cholelithiasis, cholangitis, biliary stricture, pancreatic head malignancy
- Hemolytic anemia — to detect excessive RBC destruction causing indirect hyperbilirubinemia
- Neonatal jaundice monitoring — indirect bilirubin is the critical marker; severe elevations risk kernicterus (bilirubin encephalopathy)
- Genetic hyperbilirubinemia syndromes — Gilbert, Crigler–Najjar, Dubin–Johnson, Rotor
Normal Reference Ranges
The reference ranges are displayed in the interactive table above. A brief summary:
| Test | Normal Range | Unit |
|---|---|---|
| Total bilirubin | 0.3 – 1.3 | mg/dL |
| Direct (conjugated) bilirubin | 0.0 – 0.5 | mg/dL |
| Indirect (unconjugated) bilirubin | 0.2 – 0.9 | mg/dL |
| Neonates | Age-specific nomogram | mg/dL |
Important note: Reference ranges vary by laboratory, analyzer platform, and reagent lot. Always interpret results against your institution’s validated reference intervals. Neonatal thresholds must be assessed using an age-specific (hour-of-life) nomogram rather than fixed cutoffs.
How Is Bilirubin Measured? The Methods Behind the Numbers
Understanding the measurement methods matters because they affect result interpretation and susceptibility to interference.
Total bilirubin — Vanadate oxidation method
The method of choice on most modern automated analyzers (e.g., Roche cobas, Beckman Coulter AU series) is vanadate (V⁵⁺) oxidation. Vanadate ions oxidize bilirubin to biliverdin, causing a measurable decrease in absorbance at approximately 450 nm. The magnitude of this absorbance drop is directly proportional to bilirubin concentration.
Key advantages over older diazo-based total bilirubin methods:
- Significantly less susceptible to interference from hemolysis, lipemia, and icterus
- Faster reaction kinetics, ideal for high-throughput automation
- Excellent reproducibility and linearity across clinically relevant ranges
Direct bilirubin — Diazo (diazotization) method
Conjugated bilirubin is water-soluble and reacts directly and rapidly with diazotized sulfanilic acid to form a colored azobilirubin complex, measured photometrically. This “direct” reaction — without requiring an accelerator — is the historical basis for the naming convention of “direct” vs. “indirect” bilirubin.
Indirect bilirubin — calculated value
Indirect bilirubin is not measured independently. It is calculated as:
Indirect bilirubin = Total bilirubin − Direct bilirubin
This has an important practical implication: any pre-analytical or analytical error in either the Total or Direct measurement will propagate into the Indirect result. A spuriously high Direct bilirubin, for instance, will falsely lower the calculated Indirect value.
Clinical Interpretation
Elevated total bilirubin (hyperbilirubinemia)
Total bilirubin elevation is the trigger to investigate further with the Direct/Indirect fractionation. Causes span all three anatomical zones:
- Acute or chronic viral hepatitis (HAV, HBV, HCV, HEV)
- Cirrhosis of any etiology
- Biliary obstruction (intrinsic or extrinsic)
- Hemolytic anemia (inherited or acquired)
- Genetic syndromes (Gilbert, Crigler–Najjar, Dubin–Johnson, Rotor)
- Drug-induced liver injury (DILI) — hundreds of agents implicated
- Sepsis (multifactorial)
- Total parenteral nutrition (TPN)-associated cholestasis
Elevated direct bilirubin (conjugated hyperbilirubinemia)
A predominant rise in conjugated bilirubin localizes the defect to the liver or biliary system (hepatic or post-hepatic jaundice). The conjugation machinery is intact, but the bilirubin cannot be excreted properly.
Hepatic (intrahepatic) causes:
- Viral hepatitis (all types)
- Alcoholic hepatitis and alcoholic cirrhosis
- Non-alcoholic steatohepatitis (NASH/MASLD)
- Drug-induced liver injury
- Primary biliary cholangitis (PBC) and primary sclerosing cholangitis (PSC)
- Dubin–Johnson syndrome (impaired canalicular export protein MRP2)
- Rotor syndrome (impaired hepatic storage)
Post-hepatic (extrahepatic obstruction) causes:
- Choledocholithiasis (common bile duct stones)
- Cholangiocarcinoma or pancreatic head carcinoma
- Biliary stricture (post-surgical or inflammatory)
- Acute cholangitis
Elevated indirect bilirubin (unconjugated hyperbilirubinemia)
A predominant rise in unconjugated bilirubin points upstream — to either excess bilirubin production or impaired hepatic uptake/conjugation (pre-hepatic or hepatic deficiency).
- Hemolytic anemia — immune-mediated (AIHA), mechanical, or hereditary (sickle cell, spherocytosis, G6PD deficiency); the liver is overwhelmed by bilirubin load despite intact conjugation capacity
- Neonatal physiologic jaundice — immature UGT1A1 activity; peaks around day 3–5 of life
- Gilbert syndrome — the most common hereditary cause (~5–10% of population); mild, benign UGT1A1 promoter variant; often identified incidentally on routine LFTs
- Crigler–Najjar syndrome types I and II — severe UGT1A1 deficiency; Type I is life-threatening without liver transplantation
- Ineffective erythropoiesis — as in thalassemia major
Decreased bilirubin levels
Low bilirubin values are rarely clinically significant. They can be seen in:
- Iron deficiency anemia — reduced RBC turnover and therefore less heme to break down
- Certain medications or supplements (e.g., high-dose ascorbic acid can falsely lower results by interfering with some assay chemistries)
- Individuals with naturally low-normal baseline values
Isolated low bilirubin in the absence of other findings generally does not require clinical action.
Precautions and Limitations
Even a technically excellent bilirubin result can be misleading if pre-analytical and analytical variables are ignored.
Hemolysis (in vitro): While the vanadate oxidation method is relatively resistant, significant in-vitro hemolysis (e.g., from difficult venipuncture or delayed processing) can still affect total bilirubin. Note that in-vivo hemolysis raises bilirubin legitimately, while in-vitro hemolysis is a specimen artifact — always check the serum index on your analyzer.
Lipemia: Severe lipemia interferes with photometric assays generally. Modern analyzers use lipemia indices to flag or correct; however, extremely lipemic specimens may require ultracentrifugation.
Drug interference:
- Rifampicin (rifampin) displaces bilirubin from albumin and competes for hepatic uptake, causing transient indirect hyperbilirubinemia — a pharmacological, not pathological, effect
- High-dose vitamin C (ascorbic acid) can suppress bilirubin readings in certain assay systems
- Nitrites (e.g., from urinary tract infections with contaminated specimens) may interfere
δ-Bilirubin (biliprotein): In prolonged cholestasis, a fraction of conjugated bilirubin covalently binds to albumin, forming δ-bilirubin. This fraction is included in total bilirubin but behaves variably in direct bilirubin assays. Its long half-life (~18 days, matching albumin) explains why bilirubin can remain elevated for weeks after biliary obstruction is relieved — a clinically important phenomenon that can falsely suggest ongoing disease.
The indirect value is a calculated difference, not a direct measurement. Errors in either Total or Direct determination propagate into the calculated Indirect result. A very low Direct bilirubin reading (near the assay’s lower limit of detection) can introduce proportionally large relative errors in the Indirect fraction.
Disclaimer: A single bilirubin result should never be used in isolation for diagnosis. Results must always be interpreted in the full clinical context — alongside other LFTs (ALT, AST, ALP, GGT), imaging findings, patient history, medications, and symptoms. This article is for educational purposes and does not constitute medical advice. Please consult a qualified healthcare provider.
Specialist’s Perspective and Conclusion
In my practice, the bilirubin panel is one of the most interpretively rich yet frequently underutilized tools we have. Many clinicians treat it as a single number — “the bili is up” — when in reality, the pattern across Total, Direct, and Indirect fractions tells a story that points directly at the underlying mechanism.
A practical framework I recommend: when you see an elevated total bilirubin, immediately ask two questions. First, which fraction predominates? Second, does the clinical picture fit? Isolated indirect hyperbilirubinemia in an otherwise healthy young adult with mild LFT changes after a viral illness is almost certainly Gilbert syndrome — no further workup needed. The same indirect predominance in a patient with anemia and splenomegaly demands a hemolysis workup. Dominant direct hyperbilirubinemia in an elderly patient with painless jaundice and weight loss is a biliary malignancy until proven otherwise.
From the laboratory side, I emphasize that the shift to vanadate oxidation for total bilirubin measurement on high-throughput platforms represents a genuine analytical advancement — particularly its robustness against the hemolysis and lipemia interference that plagued older diazo-based methods. It has improved result reliability meaningfully, especially in ICU and neonatal populations where specimen quality is often suboptimal.
Key takeaway: Always fractionate. Always correlate. And always remember that the indirect bilirubin is a calculated estimate — its reliability is only as good as the accuracy of the Total and Direct measurements from which it is derived.
Author Profile
This post was authored by a physician board-certified in Laboratory Medicine (MD.PhD.) with specialty expertise in clinical chemistry, point-of-care testing, and laboratory quality management. The author has extensive experience interpreting biochemical panels in both academic medical center and community hospital settings, with a focus on translating complex laboratory science into actionable clinical guidance.
[MD.phD.] Procalcitonin (PCT) Test – MedLab Insight
[MD.PhD.] BNP vs NT-proBNP (2026) – MedLab Insight
Some images are generated by AI.
References
- Fevery, J. (2008). Bilirubin in clinical practice: A review. Liver International, 28(5), 592–605. https://doi.org/10.1111/j.1478-3231.2008.01716.x
- Kaplan, M. M., & Hammaker, L. (1978). Bilirubin metabolism: An overview. Hepatology, 9, 135–142.
- Mayo Clinic Laboratories. (2024). Bilirubin, total and direct, serum. https://www.mayocliniclabs.com
- UpToDate. (2024). Approach to the patient with jaundice or asymptomatic hyperbilirubinemia. Wolters Kluwer. https://www.uptodate.com
- Roche Diagnostics. (2023). BILIRUBINT2 (Vanadate oxidation): Package insert. Cobas 8000 modular analyzer series.
- National Institutes of Health – MedlinePlus. (2023). Bilirubin blood test. U.S. National Library of Medicine. https://medlineplus.gov/lab-tests/bilirubin-blood-test/
- Bosma, P. J. (2003). Inherited disorders of bilirubin metabolism. Journal of Hepatology, 38(1), 107–117. https://doi.org/10.1016/S0168-8278(02)00359-8