
[MD.PhD.] Blood Culture Testing (2026)
Blood Culture: A Laboratory Medicine Specialist’s Complete Guide to Sepsis Diagnosis and Interpretation
Written by a Board-Certified Laboratory Medicine Specialist (MD.PhD.)
Blood culture is the gold standard diagnostic test for bacteremia and sepsis — two of the most time-critical emergencies in modern medicine. As a Laboratory Medicine Specialist, I have seen the blood culture result transform a clinician’s approach to a critically ill patient more dramatically than almost any other single test: it converts empirical treatment into targeted, evidence-based therapy, and in doing so, it saves lives. This post covers everything clinicians and informed patients should understand about blood culture — what it tests for, how it is performed, how to distinguish true bacteremia from contamination, how antibiotic susceptibility testing is integrated, and where the most consequential pre-analytical errors occur.
What Is the Blood Culture Test and Why Is It Ordered?
A blood culture is a microbiological test in which a volume of the patient’s blood is inoculated into specialized growth media (broth bottles) and incubated under controlled conditions to detect viable bacteria or fungi circulating in the bloodstream. Because blood is normally a sterile body fluid, any organism that grows in a properly collected blood culture represents either a genuine pathogen — or, critically, a contaminant introduced during collection. Distinguishing between these two possibilities is one of the core interpretive challenges of the test.
The four major clinical indications for blood culture:
1. Early diagnosis of bacteremia and sepsis Sepsis mortality is directly tied to the speed of appropriate antibiotic initiation. The Surviving Sepsis Campaign guidelines recommend that blood cultures be collected before the first antibiotic dose whenever doing so does not delay treatment by more than 45 minutes. A positive culture with a confirmed organism and sensitivity data allows de-escalation from broad-spectrum empirical therapy to targeted treatment — reducing toxicity, cost, resistance pressure, and mortality.
2. Source identification and systemic spread confirmation Local infections — pneumonia, urinary tract infection, meningitis, peritonitis, cholangitis — frequently seed the bloodstream even before clinical signs of systemic infection are apparent. A positive blood culture in this context confirms hematogenous dissemination and escalates the clinical urgency of source control.
3. Antibiotic susceptibility testing (AST) Once an organism grows in blood culture, the laboratory performs antibiotic susceptibility testing on the isolated strain. This produces a definitive antibiogram that guides optimal antibiotic selection — the minimum inhibitory concentration (MIC) data generated here is among the most clinically actionable information the laboratory produces.
4. Treatment monitoring and clearance documentation In conditions such as Staphylococcus aureus bacteremia, infective endocarditis, candidemia, and catheter-related bloodstream infection (CLABSI), serial blood cultures are drawn every 24–48 hours to document clearance of the organism from the bloodstream. Persistent bacteremia despite appropriate antibiotics mandates investigation for a focus of undrained infection or endovascular source.
Blood Culture Result Interpretation
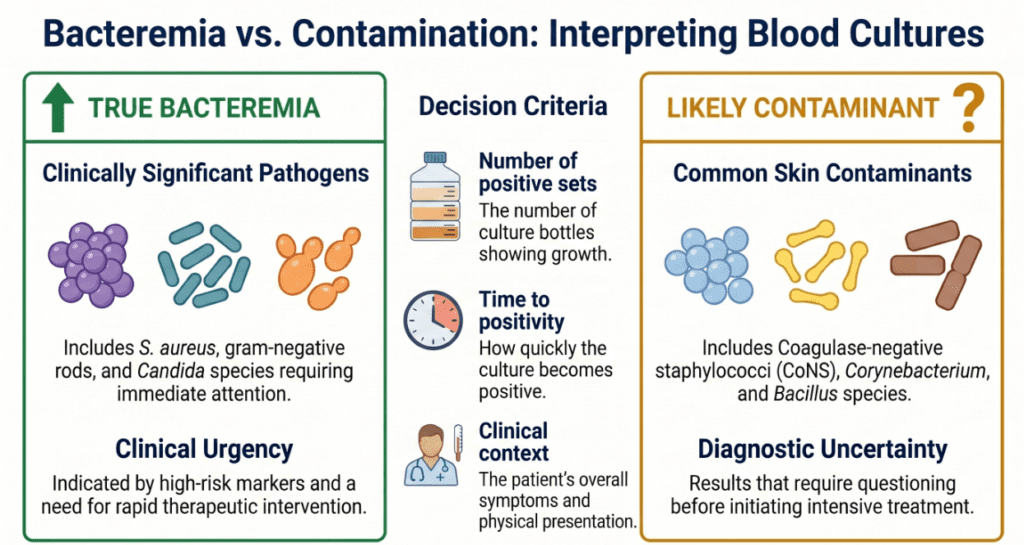
Blood culture is a qualitative test — results are reported as positive (growth detected) or negative (no growth within the incubation period). There is no numerical reference range in the conventional sense. The critical interpretive framework is not simply positive vs. negative, but true bacteremia vs. contaminant.
| Result | Organism Class | Clinical Interpretation |
|---|---|---|
| Positive | S. aureus, gram-negative rods (E. coli, Klebsiella), Streptococcus pneumoniae | Almost always true bacteremia; treat urgently |
| Positive | Candida spp. | Essentially never a contaminant; initiate antifungal therapy immediately |
| Positive | Coagulase-negative staphylococci (CoNS) | Most commonly a contaminant; true infection if multiple sets positive, CVC present, or immunocompromised host |
| Positive | Corynebacterium, Bacillus (non-anthracis), Propionibacterium acnes | Usually skin flora contaminants; clinical correlation essential |
| Negative (5-day incubation) | N/A | Does not exclude infection; sensitivity reduced by prior antibiotics, low-volume collection, or fastidious organisms |
| Negative (extended incubation, 7–14 days) | N/A | Appropriate for suspected fungal infection or fastidious organisms (HACEK, Brucella, etc.) |
Note: Blood culture interpretation is not a standalone laboratory exercise. Every result — positive or negative — must be integrated with the clinical presentation, collection technique, the number of positive sets, and the time to positivity. No single result should drive clinical decisions without this context.
How Blood Culture Is Performed: From Collection to Antibiogram
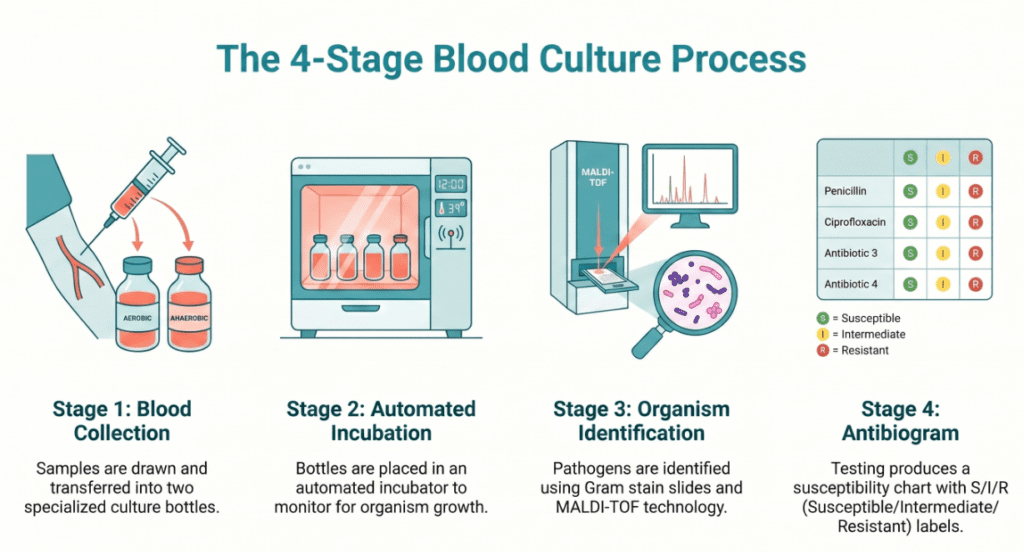
The blood culture process is a multi-stage workflow that begins at the bedside and ends with a full antibiogram. Pre-analytical errors at the bedside are the leading cause of both false-negative results and contamination — both of which carry real patient harm.
Step 1 — Blood Collection
Volume and set composition:
- The standard adult collection is two sets per draw event, each set consisting of one aerobic bottle and one anaerobic bottle
- Each bottle should receive 8–10 mL of blood (adults); lower volumes substantially reduce sensitivity — for every 1 mL below the recommended volume, sensitivity for bacteremia detection decreases measurably
- Pediatric bottles accept smaller volumes (1–3 mL); volume per kilogram of body weight guides collection in neonates and infants
Skin antisepsis — the single most modifiable determinant of contamination rate:
- Standard protocol: 70% isopropyl alcohol followed by chlorhexidine gluconate (≥0.5%) or povidone-iodine
- Allow antiseptic to dry completely before puncture (typically 30–60 seconds for chlorhexidine)
- Do not re-palpate the venipuncture site after antisepsis without re-cleansing
- A contamination rate above 3% is considered a quality indicator failure in most accredited laboratories
Peripheral vein vs. central venous catheter (CVC):
- Peripheral venipuncture is strongly preferred; CVC-only collection increases contamination risk and confounds the interpretation of catheter-associated infection
- When CLABSI is suspected, simultaneous draw from a peripheral vein and from the CVC lumen (with careful documentation of draw time) allows calculation of differential time to positivity — the most rigorous method for diagnosing CLABSI
Step 2 — Automated Continuous Monitoring Incubation
Inoculated bottles are loaded into an automated blood culture system (e.g., BacT/ALERT, BACTEC FX, Versa TREK). These platforms:
- Incubate bottles at 35–37°C with continuous agitation to maximize organism growth
- Monitor every 10 minutes for metabolic signals of growth (CO₂ production in BACTEC; colorimetric sensor changes in BacT/ALERT)
- Flag positive bottles with an alarm within minutes of detection threshold being crossed
- Standard incubation: 5 days for routine bacterial pathogens; extended to 7–14 days for suspected fungemia, Brucella, or HACEK organisms
Resin-containing bottles (e.g., BACTEC Plus Aerobic/F) are specifically designed for patients who have already received antibiotics — the resin beads adsorb residual antibiotic molecules from the blood, allowing organisms that would otherwise be suppressed to grow. These should be ordered whenever antibiotic administration has preceded collection.
Step 3 — Organism Identification
When a bottle signals positive, the laboratory subcultures the broth to solid media, performs Gram stain, and initiates identification. Modern laboratories use:
- MALDI-TOF mass spectrometry — identifies organisms to the species level within minutes directly from the positive broth or colony; has transformed turnaround time compared to traditional biochemical methods
- Molecular panels (e.g., BioFire FilmArray BCID2) — multiplex PCR directly from positive blood culture broth; identifies ~40+ organisms and key resistance genes (MRSA, VRE, ESBL, KPC, etc.) within one hour of positivity; increasingly used to accelerate antimicrobial stewardship decisions
Step 4 — Antibiotic Susceptibility Testing (AST)
Once the organism is identified, AST is performed on the isolated strain:
| Method | Principle | Output | Common Use |
|---|---|---|---|
| Disk diffusion (Kirby-Bauer) | Antibiotic disk placed on inoculated agar; inhibition zone diameter measured | S / I / R category | Widely available; CLSI/EUCAST standardized |
| Automated MIC (VITEK 2, MicroScan) | Serial dilution in microtiter wells; turbidity read automatically | MIC value + S/I/R | Most common in large hospitals; rapid, reproducible |
| E-test (gradient strip) | Antibiotic gradient on agar strip; MIC read at growth inhibition ellipse | Precise MIC value | Confirmatory testing; unusual organisms or antibiotics |
Susceptibility categories follow internationally harmonized breakpoints from CLSI (Clinical and Laboratory Standards Institute) or EUCAST (European Committee on Antimicrobial Susceptibility Testing).
Clinical Significance: Conditions Associated With Positive Blood Culture
True Bacteremia and Fungemia — Conditions Requiring Urgent Response
A confirmed positive blood culture is never a benign result. The following conditions most commonly present with positive blood cultures:
- Sepsis and septic shock — any organism; prognosis worsens with each hour of delayed appropriate antibiotic therapy
- Infective endocarditis (IE) — particularly S. aureus, viridans streptococci, enterococci; requires prolonged intravenous antibiotics and often surgery
- Catheter-related bloodstream infection (CLABSI) — S. aureus, CoNS, Candida; mandates catheter removal in most cases
- Bacteremic pneumonia — S. pneumoniae, S. aureus, gram-negative rods; blood culture positivity worsens prognosis
- Urosepsis — E. coli, Klebsiella, Enterococcus; one of the most common sources of gram-negative bacteremia
- Spontaneous bacterial peritonitis (SBP) — E. coli, Klebsiella, streptococci in cirrhotic patients
- Meningitis with bacteremia — N. meningitidis, S. pneumoniae, Listeria; blood culture may be positive even when CSF culture is negative
- Candidemia — Candida albicans and non-albicans species; mortality exceeds 40% without prompt antifungal therapy; ophthalmology consult mandatory to exclude endophthalmitis
Organism-Specific Clinical Urgency
| Organism | Clinical Significance | Mandatory Response |
|---|---|---|
| Staphylococcus aureus | Always a true pathogen; high risk of endocarditis and metastatic infection | Echocardiogram; 14-day minimum IV therapy; repeat cultures |
| Candida spp. | Essentially zero contamination rate | Antifungal therapy within hours; ophthalmology consult; echocardiogram |
| Gram-negative rods (E. coli, Klebsiella, Pseudomonas) | Usually true bacteremia from urinary, biliary, or GI source | Source identification and control; AST-guided de-escalation |
| Streptococcus pneumoniae | Pneumonia, meningitis, or primary bacteremia | Lumbar puncture to exclude meningitis |
| CoNS (e.g., S. epidermidis) | Contaminant in most cases; true infection in CVC patients | Correlate with TTP, number of positive sets, clinical context |
Precautions and Limitations
Pre-Analytical Factors That Reduce Sensitivity (False-Negative Results)
- Antibiotic administration before collection — the most impactful single variable; organisms may be suppressed below detection threshold; always draw blood cultures before the first antibiotic dose when clinically feasible; use resin-containing bottles when collection after antibiotics is unavoidable
- Insufficient blood volume — collecting 3–4 mL instead of 8–10 mL per bottle can reduce sensitivity by 20–40%; volume is non-negotiable
- Too few sets collected — a single set detects approximately 65–75% of bacteremias; two sets increase sensitivity to 80–90%; three sets approach 96–99%
- Delayed transport or incorrect temperature — bottles should reach the incubator within two hours of collection; prolonged room-temperature storage before loading reduces viability of fastidious organisms
Factors That Increase Contamination (False-Positive Results)
- Inadequate skin antisepsis or failure to allow antiseptic to dry
- Re-palpation of the venipuncture site after cleaning
- Collection from existing intravenous catheters without a paired peripheral draw
- Use of single gloves that have touched non-sterile surfaces immediately before collection
The Time-to-Positivity (TTP) Interpretive Tool
TTP — the time from bottle loading to instrument-detected positivity signal — is a valuable but underutilized interpretive parameter:
- TTP < 12 hours: Strongly suggests high-grade true bacteremia with large organism burden
- TTP 12–48 hours: Intermediate; most true bacteremias fall in this range
- TTP > 72 hours: Increases suspicion for contamination, particularly with CoNS or Corynebacterium; also seen with fastidious organisms growing slowly
- Differential TTP (CVC vs. peripheral): If the CVC draw signals positive ≥2 hours before the peripheral draw, CLABSI is strongly supported
Critical reminder: No blood culture result — positive or negative — should ever be interpreted in isolation. A result reported without the clinical story, collection details, and organism identity is incomplete information. Do not make irreversible clinical decisions based on a single blood culture result alone.
Specialist’s Perspective and Conclusion
After years working at the intersection of the laboratory and the bedside, I want to share the insight that has most shaped my approach to blood culture: the result you receive is only as good as the specimen you sent.
I have reviewed countless cases where a patient had genuine bacteremia and a negative blood culture — not because the organism was absent, but because antibiotics were started first, or because a single low-volume set was collected from a CVC. And I have reviewed equally many cases where a CoNS in one bottle triggered days of unnecessary vancomycin therapy because the contamination vs. true infection framework was not applied at the time of result reporting.
The most impactful quality improvements in blood culture diagnostics are not technological — they are behavioral. Training nursing and medical staff in proper antiseptic technique, enforcing adequate blood volumes, and establishing clear clinical protocols for pre-antibiotic collection are the interventions with the greatest return.
From an interpretive standpoint, my strongest recommendation is to treat S. aureus bacteremia with the same gravity as a myocardial infarction. It is never incidental, it never resolves without treatment, and it frequently disseminates to heart valves, bones, and joints. Every S. aureus blood culture positive result should trigger an automatic infectious disease consultation protocol — ideally a standing order pathway between the laboratory and infectious disease service.
The integration of rapid molecular diagnostics (MALDI-TOF and multiplex PCR panels) directly from positive blood culture broth has dramatically shortened the time from positivity to targeted therapy in hospitals that have adopted these platforms. If your institution does not yet have this capability, it is among the highest-value investments a clinical microbiology laboratory can make.
Key takeaway: Blood culture is the diagnostic cornerstone of sepsis management. Collect two sets, collect enough volume, collect before antibiotics whenever possible, and apply the contamination vs. true bacteremia framework rigorously to every positive result. The laboratory and the clinical team must work as one to translate this result into timely, targeted, life-saving therapy.
Author Profile
This article was authored by a board-certified specialist in Laboratory Medicine (MD.PhD.) with clinical expertise in clinical microbiology, antimicrobial stewardship, and critical care diagnostics. The author has extensive experience in designing blood culture quality improvement programs and in the rapid diagnostic workup of sepsis and bloodstream infections.
[MD.PhD.] Anaerobic Culture Test (2026) – MedLab Insight
[MD.PhD.] Stool Hb Quantitative Test (2026) – MedLab Insight
Some images are generated by AI.
References
- Surviving Sepsis Campaign. (2021). Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Medicine, 47(11), 1181–1247. https://doi.org/10.1007/s00134-021-06506-y
- Baron, E. J., Miller, J. M., Weinstein, M. P., et al. (2013). A guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2013 recommendations by the Infectious Diseases Society of America. Clinical Infectious Diseases, 57(4), e22–e121. https://doi.org/10.1093/cid/cit278
- Weinstein, M. P., & Towns, M. L. (2020). Blood cultures: Principles and practices. In Manual of clinical microbiology (12th ed.). ASM Press.
- Pappas, P. G., Kauffman, C. A., Andes, D. R., et al. (2016). Clinical practice guideline for the management of candidiasis: 2016 update by the IDSA. Clinical Infectious Diseases, 62(4), e1–e50. https://doi.org/10.1093/cid/civ933
- Bai, A. D., Lo, C. K. L., Komorowski, A. S., et al. (2020). Staphylococcus aureus bacteremia mortality: A systematic review and meta-analysis. Infectious Diseases, 52(2), 79–95.
- Clinical and Laboratory Standards Institute (CLSI). (2022). Performance standards for antimicrobial susceptibility testing (32nd ed.; CLSI supplement M100). CLSI.
- UpToDate. (2025). Blood cultures for the detection of bacteremia. Wolters Kluwer. https://www.uptodate.com