
[MD.PhD.] Anaerobic Culture Test (2026)
Anaerobic Culture: A Laboratory Medicine Specialist’s Complete Guide to Diagnosis and Interpretation
Written by a Board-Certified Laboratory Medicine Specialist (MD.PhD.)
Anaerobic bacteria are among the most frequently overlooked pathogens in clinical microbiology — yet they are responsible for some of the most dangerous, and sometimes fatal, infections encountered in medicine. As a Laboratory Medicine Specialist, I have seen firsthand how a missed anaerobic culture can delay appropriate antibiotic therapy for days, with devastating consequences in conditions like necrotizing fasciitis, intra-abdominal sepsis, or Clostridium-associated gas gangrene.
The anaerobic culture test grows bacteria that cannot survive in the presence of oxygen, detecting organisms that a standard aerobic culture will entirely miss. This post covers the purpose of anaerobic culture, which specimens are appropriate, how the test is performed, how to interpret results — including the critical nuance of distinguishing contamination from true infection — and where this test fits in the broader clinical picture.
What Is the Anaerobic Culture Test and Why Is It Ordered?
An anaerobic culture is a specialized microbiological test designed to detect bacteria that grow only in the absence — or near-absence — of oxygen. These organisms, called obligate anaerobes, inhabit normal human mucosal surfaces in enormous numbers (the large intestine alone harbors roughly 10¹¹ anaerobes per gram of contents), but when they gain access to normally sterile body sites through trauma, surgery, or tissue ischemia, they can cause severe, life-threatening infections.
Because standard aerobic culture incubators expose organisms to atmospheric oxygen, anaerobic bacteria die before colonies can form. Without a dedicated anaerobic culture setup, these pathogens are simply invisible to the laboratory — and by extension, to the treating clinician.
The major anaerobic pathogens and where they cause disease:
- Bacteroides fragilis group — the most clinically significant anaerobe; dominant in intra-abdominal and pelvic infections; intrinsically resistant to many penicillins
- Clostridium species — including C. perfringens (gas gangrene), C. difficile (colitis), C. botulinum, and C. tetani
- Fusobacterium species — head, neck, and pulmonary infections; associated with Lemierre’s syndrome
- Peptostreptococcus / Finegoldia magna — polymicrobial wound and pelvic infections
- Prevotella and Porphyromonas species — oral, dental, and aspiration pneumonia
Clinical indications — when a physician orders anaerobic culture:
- Deep tissue infections, surgical site infections, or wounds with foul-smelling discharge (malodor strongly suggests anaerobic involvement)
- Intra-abdominal infections: appendicitis, diverticulitis, peritonitis, liver abscess
- Pelvic infections: pelvic inflammatory disease (PID), postpartum endometritis, tubo-ovarian abscess
- Aspiration pneumonia or lung abscess (oral anaerobes aspirated into the lower airway)
- Diabetic foot infections, decubitus ulcers, or any polymicrobial wound with necrotic tissue
- Necrotizing fasciitis or gas gangrene (surgical emergency; culture supports pathogen identification)
- Bacteremia in patients with a gastrointestinal or hepatobiliary source
- Head and neck deep space infections, odontogenic abscesses, parotitis
Result Interpretation: Positive vs. Negative in Context
Unlike quantitative biomarker tests, anaerobic culture does not produce a numerical reference range — it is a qualitative (positive/negative) microbiological test. Interpretation depends critically on anatomical site, specimen type, and clinical context.
| Result | Specimen Source | Clinical Interpretation |
|---|---|---|
| Negative (no growth) | Any sterile site | Does not exclude anaerobic infection — see limitations below |
| Positive — known anaerobe isolated | Deep tissue, abscess, sterile fluid | Clinically significant; guide antibiotic therapy accordingly |
| Positive — mixed flora (B. fragilis + aerobe) | Intra-abdominal, wound | Polymicrobial infection; both components require coverage |
| Positive — anaerobe from mucosal surface | Oropharynx, rectum, vagina | Likely colonizer, not pathogen; interpret with clinical context |
| Bacteroides bacteremia | Blood culture | High clinical significance; associated with elevated mortality |
| Clostridium perfringens | Deep wound with gas | Surgical emergency; gas gangrene must be excluded urgently |
Note: A negative anaerobic culture result does not rule out anaerobic infection. Interpretation must always incorporate specimen quality, transport conditions, clinical stage, and antibiotic history. Reference values for microbiology cultures are site- and organism-specific and may vary by laboratory protocol.
How the Anaerobic Culture Is Performed
The anaerobic culture workflow differs substantially from routine aerobic culture, beginning before the specimen even reaches the laboratory.
Specimen Collection: The Most Critical Variable
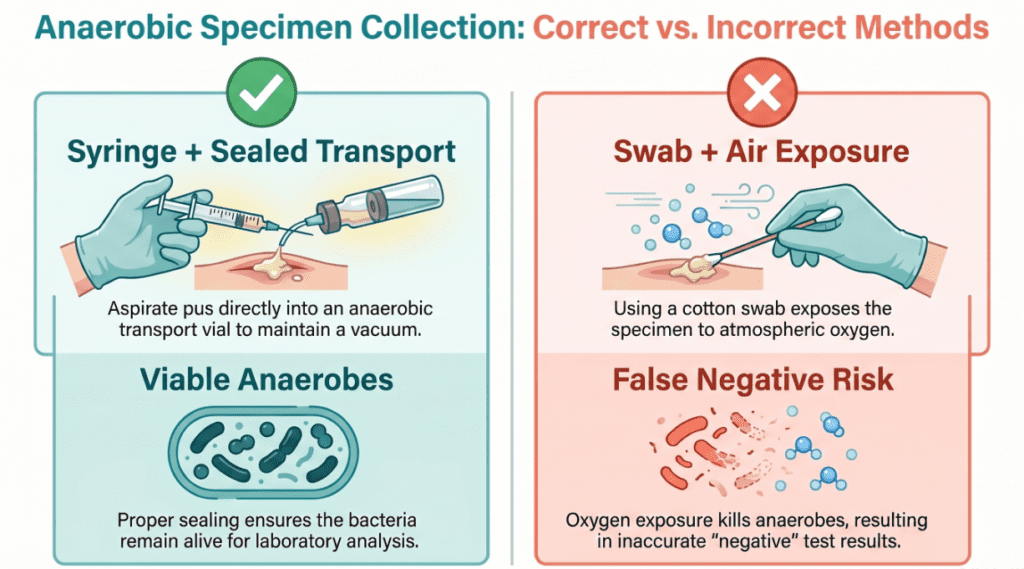
The cardinal rule of anaerobic culture is minimize oxygen exposure from the moment of collection to the moment of plating. Anaerobic bacteria begin dying within minutes of oxygen contact, making pre-analytical handling the single most important determinant of culture sensitivity.
Appropriate specimen types (ranked by quality):
| Specimen | Recommendation | Rationale |
|---|---|---|
| Aspirated pus or abscess fluid (syringe) | Strongly preferred | Excludes air; high organism load; optimal for anaerobes |
| Surgical tissue biopsy | Excellent | Anaerobes embedded in tissue survive transport better |
| Peritoneal / pleural / synovial fluid | Excellent | Sterile site specimen; high clinical relevance |
| Bile, surgical drainage fluid | Appropriate | Submit in anaerobic transport vial immediately |
| Blood (anaerobic blood culture bottle) | Essential for suspected bacteremia | Purpose-built resin-containing broth eliminates oxygen |
| Swab from wound surface | Not recommended | Rapid oxygen exposure; poor recovery; high false-negative rate |
| Sputum, urine, skin surface | Not appropriate | Heavy normal flora contamination; anaerobes are commensals here |
Transport requirements:
- Use purpose-built anaerobic transport media (e.g., Port-A-Cul, Anaerobic Transport Medium)
- Transport to the laboratory within 15–30 minutes where possible; two-hour maximum
- Never refrigerate anaerobic specimens — cold temperatures are additionally damaging to many anaerobes
- Never use swabs unless no alternative exists
Laboratory Processing
Once the specimen arrives, the laboratory performs the following:
- Anaerobic chamber or gas pak jar: Specimen is plated inside an environment where oxygen is chemically eliminated (hydrogen + carbon dioxide with a palladium catalyst), achieving <0.5% O₂
- Selective and non-selective media: Brucella blood agar (non-selective), phenylethyl alcohol agar (inhibits gram-negatives; selects gram-positives), Bacteroides bile esculin agar (selects Bacteroides group)
- Incubation: 35–37°C for 48–72 hours minimum; plates should be held up to 5 days before calling negative for slow-growing species
- Identification workflow: Gram stain of colonies → biochemical identification → MALDI-TOF mass spectrometry (now the gold standard for speed and accuracy) → antibiotic susceptibility testing by MIC or E-test for clinically significant isolates
Clinical Significance: Diseases and Conditions Associated With Anaerobic Infection
Conditions Where Anaerobic Culture Is Clinically Decisive
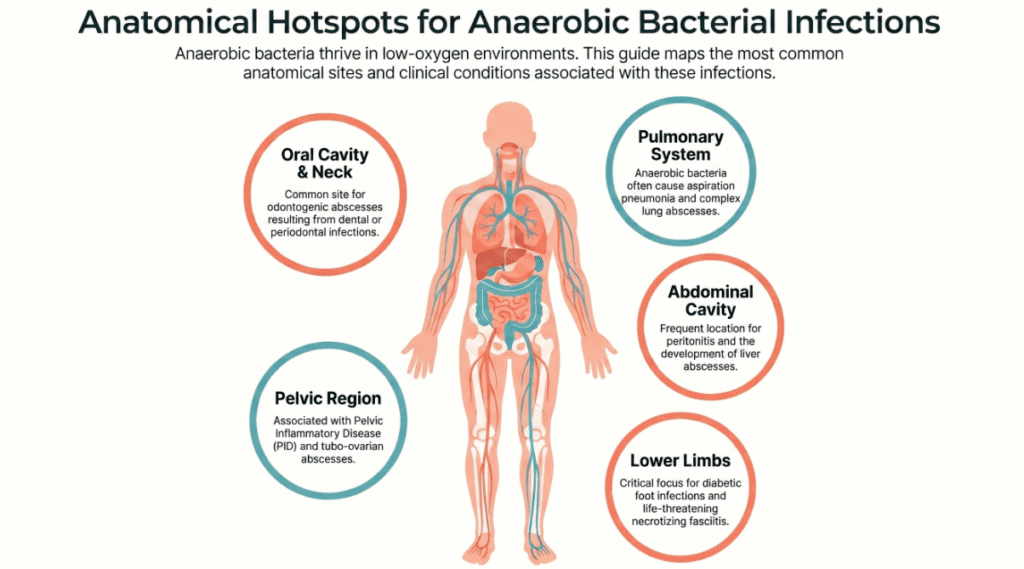
Anaerobic infections are not randomly distributed — they cluster around anatomical sites where normal anaerobic flora is abundant and can be displaced into normally sterile tissue:
Intra-abdominal and pelvic infections:
- Appendicitis with perforation and peritonitis
- Diverticulitis with abscess formation
- Liver abscess (often polymicrobial)
- Pelvic inflammatory disease and tubo-ovarian abscess
- Postpartum or post-abortion endometritis
Skin, soft tissue, and musculoskeletal infections:
- Necrotizing fasciitis (frequently polymicrobial; anaerobes nearly always present)
- Diabetic foot infections (among the most common polymicrobial anaerobic infections seen in clinical practice)
- Decubitus ulcers with deep tissue involvement
- Gas gangrene (Clostridium perfringens — a true surgical emergency)
Pulmonary infections:
- Aspiration pneumonia (oral anaerobes aspirated into dependent lung segments)
- Lung abscess (frequently mono- or polymicrobial anaerobic)
- Empyema with putrid odor
Head, neck, and dental infections:
- Odontogenic abscess and Ludwig’s angina
- Deep neck space infections
- Lemierre’s syndrome (Fusobacterium necrophorum bacteremia from pharyngitis)
- Parotitis and submandibular space infections
Bloodstream infections:
- Bacteroides bacteremia: carries high mortality; typically originates from a gastrointestinal, hepatobiliary, or pelvic source
- Clostridium bacteremia: can indicate bowel pathology, malignancy, or immunosuppression
The Polymicrobial Complexity
One of the most clinically important features of anaerobic infections is that they are rarely monomicrobial. The typical intra-abdominal abscess contains 3–5 different organisms — a mixture of anaerobes and facultative aerobes that synergize with one another. Bacteroides fragilis, for example, produces a polysaccharide capsule that enables aerobic copathogens to evade phagocytosis. This synergy means that:
- Antibiotic therapy must cover both the aerobic and anaerobic components
- Surgical source control (drainage, debridement) is often as critical as antibiotics
- Cultures from polymicrobial infections require careful clinical correlation to determine which organisms are driving pathology
Commonly used antibiotic classes for anaerobic coverage:
- Metronidazole (excellent anaerobic coverage; drug of choice for B. fragilis)
- β-lactam / β-lactamase inhibitor combinations (amoxicillin-clavulanate, piperacillin-tazobactam)
- Carbapenems (broadest spectrum; reserved for severe or resistant infections)
- Clindamycin (historically used; increasing resistance limits its utility for Bacteroides)
Precautions and Limitations
Factors that reduce anaerobic culture sensitivity and produce false-negative results:
- Oxygen exposure during collection or transport — the most common cause of false-negative anaerobic cultures; a swab left uncapped for even two minutes may lose all anaerobic viability
- Transport delay — organisms lose viability rapidly; delays beyond two hours substantially increase false-negative rates
- Prior antibiotic therapy — even a single dose of metronidazole or a carbapenem will suppress anaerobic growth; always document antibiotic history on the culture requisition
- Inappropriate specimen type — surface swabs from wounds, sputum, or voided urine are essentially useless for anaerobic culture and should not be ordered for this purpose
- Specimen volume — small-volume aspirates reduce the probability of organism recovery; whenever possible, submit all available material
Factors that complicate interpretation:
- Normal flora contamination: Mucosal surfaces (oral cavity, large bowel, vagina, skin) carry large resident anaerobic populations. Recovering Prevotella or Peptostreptococcus from a throat swab is meaningless; recovering the same organisms from a deep neck abscess aspirate is highly significant. The same organism can be a colonizer or a pathogen depending entirely on the site.
- Polymicrobial results: When two or more organisms grow together, determining the relative contribution of each to the disease process requires clinical judgment, not just laboratory data. Not every organism in a mixed culture is equally important.
- Slow growth leading to delayed reporting: Anaerobic cultures may not finalize for 5–7 days. Empirical broad-spectrum antibiotic coverage must be initiated based on clinical presentation, not held pending culture confirmation.
Critical reminder: A negative anaerobic culture result must never be used to rule out anaerobic infection in a clinically compatible presentation. If anaerobic infection is clinically suspected — particularly in the setting of foul-smelling discharge, deep tissue necrosis, or failure to respond to aerobic-only antibiotic coverage — empirical anaerobic coverage should be continued regardless of culture results.
Specialist’s Perspective and Conclusion
In my years of laboratory medicine practice, anaerobic culture is one of the tests where pre-analytical errors do the most damage — and where the gap between what clinicians intend to order and what actually reaches the laboratory in usable condition is widest. The most important message I can offer clinicians is this: the quality of the anaerobic culture result is determined in the first five minutes after specimen collection, not in the laboratory.
A perfectly executed culture protocol cannot compensate for a swab that sat on a counter for an hour. When you suspect an anaerobic infection, commit to it: use a syringe, aspirate as much material as possible, inject it directly into an anaerobic transport vial, and send it immediately. That single decision has more impact on patient outcome than almost any analytical variable within the laboratory’s control.
I also want to emphasize the clinical danger of anchoring exclusively on culture results in anaerobic infections. Because of the organism’s sensitivity to oxygen, transport conditions, and prior antibiotics, a negative culture has substantially less reassuring power than a negative culture for most aerobes. In the right clinical context — intra-abdominal sepsis, necrotizing soft tissue infection, lung abscess — empirical anaerobic coverage is not optional, and it should not be withdrawn based solely on a negative culture.
Key takeaway: Anaerobic culture is an indispensable diagnostic tool for deep tissue, intra-abdominal, pelvic, and pulmonary infections. Its sensitivity is entirely dependent on correct specimen type and handling. Interpret results within the full clinical context — anatomical site, specimen quality, polymicrobial complexity, and the patient’s antibiotic history — and never allow a negative result to override strong clinical suspicion of anaerobic infection.
Author Profile
This article was authored by a board-certified specialist in Laboratory Medicine (MD.PhD.) with clinical expertise in clinical microbiology, infectious disease diagnostics, and antimicrobial stewardship. The author’s academic and clinical work focuses on translating complex microbiological results into actionable guidance for clinicians managing severe and complex infections.
[MD.PhD.] Stool Hb Quantitative Test (2026) – MedLab Insight
[MD.PhD.] Bordetella pertussis Culture (2026) – MedLab Insight
References
- Brook, I. (2020). Anaerobic infections: Diagnosis and management. Infectious Disease Clinics of North America, 34(4), 833–851. https://doi.org/10.1016/j.idc.2020.08.001
- Goldstein, E. J. C., Citron, D. M., & Tyrrell, K. L. (2013). Comparative in vitro activities of oritavancin against 209 aerobic and anaerobic pathogens isolated from skin and soft tissue animal and human bite wound infections. Antimicrobial Agents and Chemotherapy, 57(9), 4277–4282.
- Murray, P. R., Rosenthal, K. S., & Pfaller, M. A. (2021). Medical microbiology (9th ed.). Elsevier.
- Murdoch, D. A. (1998). Gram-positive anaerobic cocci. Clinical Microbiology Reviews, 11(1), 81–120. https://doi.org/10.1128/CMR.11.1.81
- Clinical and Laboratory Standards Institute (CLSI). (2018). Methods for antimicrobial susceptibility testing of anaerobic bacteria (9th ed.; CLSI document M11-A9). CLSI.
- UpToDate. (2025). Overview of anaerobic bacteria. Wolters Kluwer. https://www.uptodate.com
- Baron, E. J., Miller, J. M., Weinstein, M. P., et al. (2013). A guide to utilization of the microbiology laboratory for diagnosis of infectious diseases: 2013 recommendations. Clinical Infectious Diseases, 57(4), e22–e121. https://doi.org/10.1093/cid/cit278