
[MD.PhD.] Stool Hb Quantitative Test (2026)
Understanding the Stool Hemoglobin Quantitative Test (Stool Hb / qFIT): A Laboratory Medicine Specialist’s Guide
Written by a Board-Certified Laboratory Medicine Specialist (MD.PhD.)
Colorectal cancer remains one of the most preventable cancers — yet it kills hundreds of thousands globally each year, largely because it goes undetected in its early, curable stages. The Stool Hemoglobin Quantitative Test (also called the quantitative Fecal Immunochemical Test, or qFIT) is the single most important non-invasive screening tool we have for detecting early colorectal cancer and high-risk polyps. This post explains what the test is, how to interpret results, its limitations, and who should be screened.
What Is the Stool Hb Quantitative Test and Why Is It Ordered?
The Stool Hb test measures the concentration of human hemoglobin (Hb) in a stool sample using immunochemical methods. Unlike older guaiac-based fecal occult blood tests (gFOBT), the immunochemical method reacts specifically to human hemoglobin — meaning dietary red meat, iron supplements, or certain vegetables do not cause false positives.
Clinical indications — why a physician orders this test:
- Colorectal cancer (CRC) screening in average-risk adults aged 45 and older
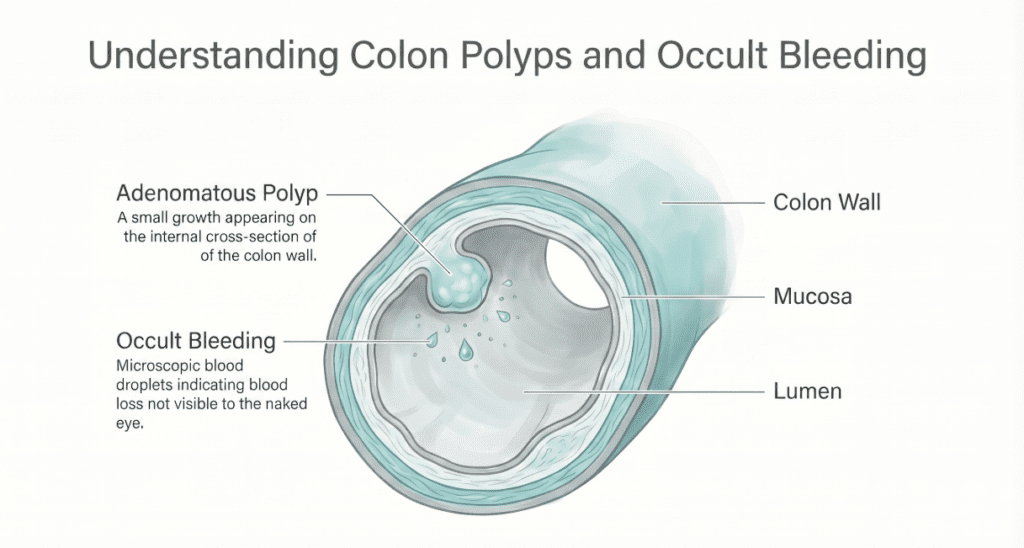
- Detection of bleeding from adenomatous or advanced colorectal polyps
- Evaluation of unexplained iron-deficiency anemia, unintentional weight loss, or altered bowel habits
- Monitoring of known inflammatory bowel disease (IBD) for mucosal bleeding activity
- Annual surveillance in high-risk individuals (first-degree family history of CRC, prior adenomas)
The test exploits the fact that colorectal tumors and large polyps are fragile, vascular lesions that bleed intermittently and at amounts too small for the naked eye to detect — but well within the detection threshold of modern immunochemical analyzers.
Normal Reference Range
Reference ranges can vary slightly between laboratories and analyzer platforms. The following represents the internationally accepted threshold used in national colorectal cancer screening programs:
| Result Category | Threshold | Unit | Interpretation |
|---|---|---|---|
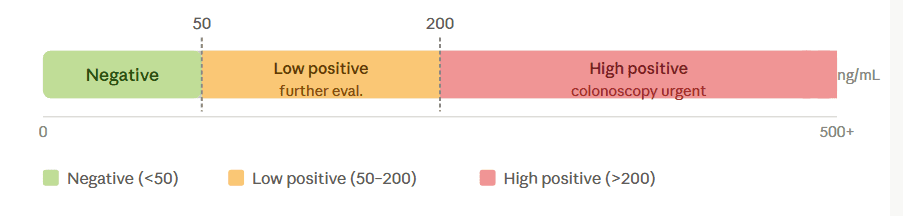
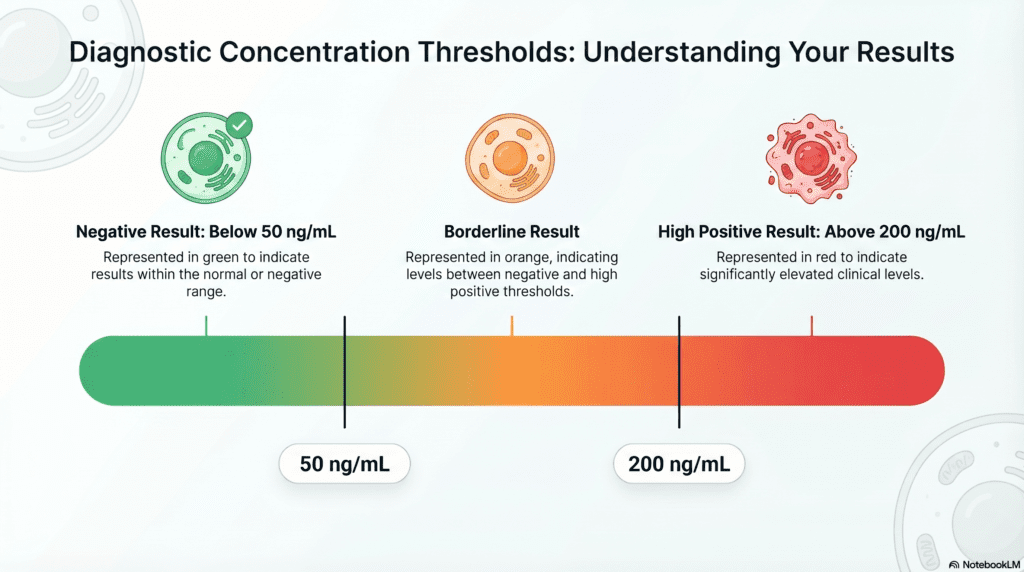
| Negative | < 50 | ng Hb/mL buffer | No significant colorectal bleeding detected |
| Positive | ≥ 50 | ng Hb/mL buffer | Significant fecal hemoglobin; colonoscopy recommended |
Note: Reference ranges may vary by laboratory and by the specific collection device used. Some programs use thresholds as low as 10 ng/mL or as high as 200 ng/mL depending on local epidemiology and endoscopy capacity. Always interpret results in the context of the reporting laboratory’s reference interval.
Higher quantitative values correlate with increasing risk: studies show that values above 200 ng/mL carry a substantially higher probability of advanced neoplasia or cancer compared to values in the 50–100 ng/mL range.
Clinical Interpretation
Elevated Results (Positive Stool Hb ≥ 50 ng/mL)
A positive result does not confirm cancer — it signals the need for diagnostic colonoscopy. Conditions that can produce a positive fecal hemoglobin result include:
- Colorectal adenocarcinoma — the primary concern; sensitivity for CRC is approximately 79–92% depending on threshold used
- Advanced adenomatous polyps — high-grade dysplasia, villous architecture, or polyps >10 mm; sensitivity ~40–50%
- Inflammatory bowel disease (IBD) — ulcerative colitis and Crohn’s disease frequently cause mucosal bleeding detectable by qFIT
- Colonic diverticulitis with mucosal erosion
- Hemorrhoids and anal fissures — a common cause of false-positive results (bleeding originates at the anorectal junction, not the colon proper)
- Colonic angiodysplasia or erosions
The magnitude of the quantitative result carries diagnostic weight. In my clinical experience, results above 200 ng/mL warrant expedited colonoscopy referral, as the positive predictive value for significant neoplasia rises markedly at higher values.
Negative Results (Stool Hb < 50 ng/mL)
A negative result substantially reduces — but does not eliminate — the probability of significant colorectal pathology. Important caveats:
- Intermittent bleeding lesions may not bleed at the moment of sample collection; a single negative test does not rule out cancer in a symptomatic patient
- Proximal (right-sided) colon cancers bleed less reliably and are detected less sensitively than left-sided lesions
- Upper GI bleeding (from stomach or small bowel) is largely digested before reaching the colon, converting hemoglobin to non-immunoreactive degradation products — these cases may produce a negative result despite significant hemorrhage
- In average-risk asymptomatic individuals, annual testing is recommended precisely because of intermittent sampling limitations
Any patient with symptoms — rectal bleeding, change in bowel habits, unexplained weight loss, iron deficiency anemia — requires colonoscopy regardless of qFIT result.
Precautions and Limitations
Pre-analytical Factors
| Factor | Impact | Recommendation |
|---|---|---|
| Menstruation | May cause false-positive result | Avoid collection during menstrual period |
| Urinary contamination of sample | Dilutes and degrades hemoglobin | Collect directly without contact with toilet water |
| Sample storage temperature | Hemoglobin degrades rapidly at room temperature | Refrigerate at 2–8°C; submit to lab within 24 hours |
| Constipation/straining | May cause anal mucosal trauma and bleeding | Note clinical context; consider repeat testing |
| Active hemorrhoidal bleeding | Anorectal blood contaminates sample | Document and consider colonoscopy directly |
Analytical and Clinical Limitations
- The immunochemical method is specific to human hemoglobin — dietary meat or certain foods do not cause interference (a key advantage over guaiac-based FOBT), and no dietary restriction is required
- The test is optimized for lower GI pathology; it is a poor screen for upper GI bleeding sources
- A single negative test does not exclude high-risk individuals from routine annual screening
- The test is a screening tool, not a diagnostic tool — colonoscopy remains the gold standard for definitive diagnosis and polypectomy
- Do not use qFIT results alone to make or rule out a cancer diagnosis; clinical correlation is mandatory
Specialist’s Perspective and Conclusion
As a laboratory medicine specialist, I want to highlight a nuance that is often missed in primary care: the quantitative value matters, not just the positive/negative call. Many laboratories report only a binary result, but when quantitative data is available, it stratifies risk. A result of 52 ng/mL and a result of 450 ng/mL both meet the “positive” threshold — but they represent very different clinical urgency. Whenever possible, request the numeric value and communicate it to the gastroenterologist.
I also frequently see patients over-reassured by a single negative qFIT result when symptoms are present. A negative test in a symptomatic patient is not a license to defer colonoscopy. The test has genuine value as an annual asymptomatic screening modality — but in the presence of symptoms, endoscopic evaluation is irreplaceable.
Key takeaway: The Stool Hb quantitative test is the best non-invasive, first-line colorectal cancer screening tool available. It is convenient, requires no dietary restriction, and has strong evidence behind it. For asymptomatic average-risk adults aged 45 and older, annual qFIT is a simple, life-saving habit. For anyone with symptoms or a positive result — proceed directly to colonoscopy without delay.
Author Profile
This article was authored by a board-certified specialist in Laboratory Medicine (MD.PhD.) with clinical and academic experience in clinical chemistry, hematology, and cancer biomarker diagnostics. The author’s work focuses on translating complex laboratory data into clinically actionable guidance for both clinicians and patients.
🦠 Bordetella pertussis Culture: A Complete Guide to Diagnosis of Whooping Cough – MedLab Insight
🧫 Anaerobic Culture Test: A Complete Guide for Clinicians and Patients – MedLab Insight
Some images are generated by AI.
References
- Imperiale, T. F., Ransohoff, D. F., Itzkowitz, S. H., et al. (2014). Multitarget stool DNA testing for colorectal-cancer screening. New England Journal of Medicine, 370(14), 1287–1297. https://doi.org/10.1056/NEJMoa1311288
- Levin, B., Lieberman, D. A., McFarland, B., et al. (2008). Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps. CA: A Cancer Journal for Clinicians, 58(3), 130–160.
- Kapidzic, A., Grobbee, E. J., Hol, L., et al. (2012). Influence of stool collection and handling on quantitative immunochemical fecal occult blood test results. Clinical Gastroenterology and Hepatology, 10(3), 272–278.
- Wolf, A. M. D., Fontham, E. T. H., Church, T. R., et al. (2018). Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA: A Cancer Journal for Clinicians, 68(4), 250–281.
- National Cancer Institute. (2024). Colorectal cancer screening (PDQ) — Health professional version. https://www.cancer.gov/types/colorectal/hp/colorectal-screening-pdq
- UpToDate. (2025). Screening for colorectal cancer: Strategies in patients at average risk. Wolters Kluwer. https://www.uptodate.com