[MD.PhD.] High-Sensitivity Troponin T (hs-TnT) Test (26)
High-Sensitivity Troponin-T (hs-TnT): A Laboratory Specialist’s Complete Guide to Interpretation
Laboratory Medicine Specialist, MD.PhD. Updated 2026
As a Laboratory Medicine Specialist, I am frequently asked about the single most important blood test we run in the emergency evaluation of chest pain. The answer is unequivocal: the high-sensitivity Troponin-T (hs-TnT) assay. This test has transformed how we diagnose acute myocardial infarction (AMI), enabling detection of even minute degrees of myocardial injury within one to two hours of symptom onset — a capability that was simply impossible with earlier-generation assays.
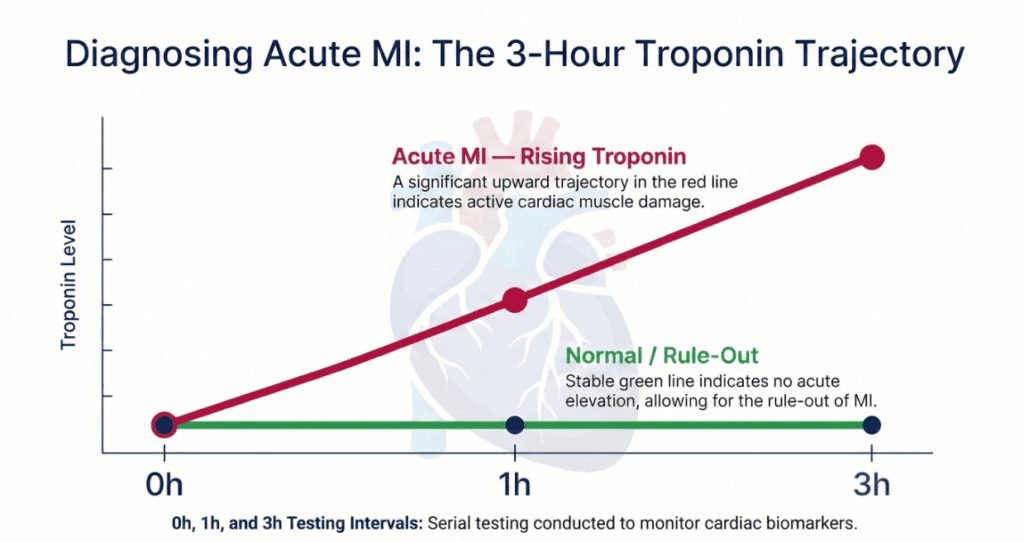
At a Glance — Featured SummaryHigh-sensitivity Troponin-T (hs-TnT) is a cardiac biomarker blood test used primarily to diagnose acute myocardial infarction (AMI) and assess myocardial injury. Using electrochemiluminescence immunoassay (ECLIA) technology, it detects troponin concentrations more than 10 times lower than conventional assays. Serial measurements at 0, 1, and 3 hours are essential for accurate interpretation — a single elevated value alone is insufficient for AMI diagnosis.
What Is Troponin-T and Why Is This Test Ordered?
Troponin is a regulatory protein complex that controls the calcium-mediated interaction between actin and myosin in cardiac and skeletal muscle cells. The complex consists of three subunits:
- Troponin T (TnT) — binds to tropomyosin and anchors the complex to the thin filament
- Troponin I (TnI) — inhibits actomyosin ATPase in the absence of calcium; the cardiac isoform (cTnI) is heart-specific
- Troponin C (TnC) — binds calcium ions and triggers muscle contraction
Critically, both cardiac TnT (cTnT) and cardiac TnI (cTnI) are expressed almost exclusively in cardiomyocytes. When these cells are damaged — by ischemia, inflammation, or any other mechanism — troponin leaks into the bloodstream, providing a highly specific signal of myocardial injury. The high-sensitivity generation of assays measures cTnT concentrations in the nanogram-per-liter range, well below the detection threshold of conventional troponin tests.
Clinical indications — when doctors order this test
- Suspected acute myocardial infarction (AMI) — the primary indication
- Chest pain evaluation in the emergency department (rapid rule-in / rule-out)
- Detection of myocardial ischemia, myocarditis, or myocardial injury
- Prognostication in heart failure and end-stage renal disease (ESRD)
- Monitoring cardiotoxicity from chemotherapy (anthracyclines, trastuzumab, etc.)
- Perioperative cardiac risk assessment in high-risk non-cardiac surgery
How the Test Is Performed: ECLIA Method
The hs-TnT assay runs on automated immunoanalyzers — most commonly the Roche Elecsys hs-Troponin T platform — using electrochemiluminescence immunoassay (ECLIA). In this method, two monoclonal antibodies sandwich the cTnT antigen. One antibody is biotin-labeled (capturing the analyte onto streptavidin-coated magnetic beads), while the other carries a ruthenium-complex label. When an electrical voltage is applied to the electrode, the ruthenium label emits light proportional to the concentration of cTnT in the sample. This technology achieves a coefficient of variation below 10% at concentrations as low as 3–5 ng/L, enabling detection of clinically meaningful subclinical injury.
- Specimen: Serum or lithium-heparin plasma (EDTA plasma is platform-dependent)
- Turnaround time: Typically 18 minutes on modern automated platforms
- Assay sensitivity: Detects cTnT at concentrations >10× lower than conventional assays
Reference Ranges (Normal Values)
Reference ranges for hs-TnT are derived from the 99th percentile of a healthy reference population, sex-stratified because women naturally have lower myocardial mass and lower baseline troponin values.
| Category | hs-TnT Threshold | Unit | Interpretation |
|---|---|---|---|
| General population (99th percentile) | ≤ 14 | ng/L (= pg/mL) | Normal |
| Women (sex-specific 99th percentile) | ≤ 9 | ng/L | Normal |
| Men (sex-specific 99th percentile) | ≤ 22 | ng/L | Normal |
| Above 99th percentile | > 14 (unsex-stratified) | ng/L | Elevated — requires clinical correlation |
| Older expression (some labs) | ≤ 0.100 | ng/mL (= μg/L) | Normal (equivalent to ≤ 100 ng/L) |
ⓘ Reference ranges vary by analyzer, reagent lot, and laboratory. Always interpret results against your institution’s established reference interval. Sex-specific cutoffs are recommended by the European Society of Cardiology (ESC) 0h/1h and 0h/2h rapid protocols.
Clinical Interpretation: What Elevated or Normal Results Mean
Elevated hs-TnT — causes and conditions
Any elevation above the 99th percentile indicates myocardial cell injury. The clinical context and the pattern of change over serial measurements determine the underlying cause:
- Acute myocardial infarction (STEMI / NSTEMI) — rapid, marked rise and fall; the most urgent cause
- Unstable angina progressing to NSTEMI — serial delta change is typically modest but definitive
- Myocarditis — sustained elevation without classic ischemic rise-and-fall kinetics; confirmed by cardiac MRI
- Heart failure (acute decompensated) — chronic low-level elevation; predicts adverse outcomes
- Rapid atrial fibrillation or other tachyarrhythmias — demand ischemia from reduced diastolic filling time
- Cardiomyopathy — dilated, hypertrophic, or stress-induced (Takotsubo) — all can mimic AMI pattern
- Pulmonary embolism — right ventricular pressure overload causes subendocardial ischemia
- Sepsis and critical illness — systemic hypoperfusion and cytokine-mediated myocardial depression
- End-stage renal disease (ESRD) — reduced clearance of troponin fragments + chronic subclinical myocardial injury
- Chemotherapy cardiotoxicity — anthracyclines, immune checkpoint inhibitors, HER2-targeted agents
AMI diagnosis requires more than one elevated value
Per ESC guidelines, AMI is diagnosed when hs-TnT exceeds the 99th percentile and a significant rise or fall (delta change) is detected on serial measurements — in conjunction with symptoms, ECG changes, or imaging evidence of new wall-motion abnormality.
Decreased hs-TnT — clinical significance
Troponin operates on a binary conceptual framework: a result below the 99th percentile is considered negative (no significant myocardial injury detected), and a value at or above it is positive. There is no clinically meaningful interpretation for values that “decrease” from one normal level to another. A declining value from an initially elevated level, however, is informative — it distinguishes evolving AMI (rise then fall) from chronic myocardial conditions that show persistently elevated but stable values (such as ESRD or heart failure).
Precautions and Limitations
01. Serial testing is mandatory
A single value cannot confirm or exclude AMI. ESC protocols require measurements at 0h and 1h (or 0h and 2h), with delta change thresholds validated for each platform.
02. Renal disease elevates baseline
Patients with ESRD or severe CKD chronically circulate troponin fragments. Knowing a patient’s habitual baseline is essential for detecting superimposed acute injury.
03. Strenuous exercise can cause mild elevation
Endurance athletes (marathon runners, cyclists) may transiently exceed the 99th percentile; values typically normalize within 24–48 hours with no clinical intervention.
04. Non-ischemic mimics
Myocarditis and Takotsubo (stress) cardiomyopathy can generate AMI-like kinetics. Differentiation requires ECG, echocardiography, and sometimes cardiac MRI.
05. A normal result does not exclude very early AMI
Within the first 60 minutes of symptom onset, hs-TnT may still be within the normal range. A repeat measurement at 1–3 hours is required before ruling out AMI.
06. Assay-specific cutoffs must be used
cTnT and cTnI assays are NOT interchangeable. Each platform (Roche, Abbott, Siemens, etc.) has its own validated 99th percentile and delta change criteria.
Important note for patients and readers
This article is intended for educational purposes. Never use a single laboratory result to self-diagnose. If you are experiencing chest pain, shortness of breath, or any cardiac symptom, seek emergency medical care immediately.
Specialist’s Perspective and Conclusion
“In my experience, the most common interpretive error I see is the over-reliance on a single hs-TnT value. Clinicians in the emergency department sometimes treat any elevation above the 99th percentile as an AMI — but the kinetics of change matter as much as the absolute number. A chronically elevated, stable hs-TnT in a dialysis patient is fundamentally different from a sharply rising value in a 55-year-old with ST-segment depression.”
— Laboratory Medicine Specialist, MD.PhD.
The high-sensitivity Troponin-T assay represents one of the most significant advances in emergency medicine biomarker science of the past two decades. Its clinical value rests on three pillars:
- Early detection: Injury detectable within 1–2 hours of symptom onset enables rapid triage and reduces time to reperfusion therapy.
- High sensitivity: A negative result at 0h and 1–2h has a negative predictive value exceeding 99% for ruling out AMI in low-risk patients, allowing safe early discharge.
- Prognostic power: Even mildly elevated hs-TnT values in heart failure or ESRD populations independently predict all-cause mortality, making it a tool for risk stratification beyond the acute setting.
The test is not a standalone oracle — it is one instrument in a clinical symphony that includes the history, physical examination, 12-lead ECG, and imaging. Used correctly, with serial measurements and validated delta-change algorithms, hs-TnT is the gold standard cardiac biomarker of our era.
Laboratory Medicine Specialist, MD.PhD.
Board-Certified in Clinical Pathology & Laboratory Medicine
The author is a board-certified physician specializing in laboratory medicine, with extensive experience in cardiac biomarker interpretation, immunoassay validation, and laboratory test utilization. Content is reviewed for accuracy against current international clinical guidelines.
[MD.PhD.] Understanding Bilirubin? (26) – MedLab Insight
[MD.PhD.] BNP vs NT-proBNP (2026) – MedLab Insight
References
- Thygesen, K., Alpert, J. S., Jaffe, A. S., et al. (2019). Fourth universal definition of myocardial infarction. European Heart Journal, 40(3), 237–269. https://doi.org/10.1093/eurheartj/ehy462
- Collet, J.-P., Thiele, H., Barbato, E., et al. (2021). 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. European Heart Journal, 42(14), 1289–1367.
- Mueller, C., Giannitsis, E., Christ, M., et al. (2016). Multicenter evaluation of a 0-hour/1-hour algorithm in the diagnosis of myocardial infarction with high-sensitivity cardiac troponin T. Annals of Emergency Medicine, 68(1), 76–87.
- Apple, F. S., Sandoval, Y., Jaffe, A. S., & Ordonez-Llanos, J. (2017). Cardiac troponin assays: Guide to understanding analytical characteristics and their impact on clinical care. Clinical Chemistry, 63(1), 73–81.
- UpToDate. (2024). Troponin testing: Clinical use. Wolters Kluwer. https://www.uptodate.com
- Mayo Clinic Laboratories. (2024). High-sensitivity troponin T test overview. https://www.mayocliniclabs.com
- Roche Diagnostics. (2023). Elecsys Troponin T hs STAT — Package insert. Roche Diagnostics GmbH.
- Cardiac troponins in patients with kidney disease – UpToDate