
[MD.phD.] CRP (C-Reactive Protein) Test
CRP (C-Reactive Protein) Test: A Specialist’s Guide to Understanding Inflammation Markers
By Laboratory Medicine Specialist, MD.phD.
Quick summary: The CRP (C-reactive protein) test is a blood test that measures a key marker of inflammation produced by the liver. It rises sharply within hours of infection, injury, or inflammatory disease — making it one of the most clinically useful acute-phase markers in modern medicine. This article covers what CRP is, how to interpret your results, what high or low levels mean, and the critical limitations clinicians must keep in mind.
1. What is the CRP test and why is it ordered?
C-reactive protein (CRP) is an acute-phase protein synthesized by the liver in response to inflammatory cytokines — most importantly interleukin-6 (IL-6). When the body experiences infection, tissue injury, or systemic inflammation, CRP concentrations rise within 6 hours, peak at 24–48 hours, and fall rapidly once the trigger resolves. This fast, reliable kinetics is what makes CRP so valuable at the bedside.
It is important to emphasize: CRP is not a diagnostic test for any single disease. Rather, it is a sensitive, non-specific signal that tells clinicians whether significant inflammation is occurring and how severe it is.
Common clinical indications
- Distinguishing bacterial from viral infections
- Monitoring severity and progression of pneumonia, sepsis, or peritonitis
- Assessing disease activity in autoimmune conditions (e.g., rheumatoid arthritis, vasculitis)
- Evaluating post-operative complications and antibiotic treatment response
- Tracking inflammation in acute pancreatitis and inflammatory bowel disease
- Supporting risk stratification for cardiovascular disease (using high-sensitivity CRP, hs-CRP)
2. Qualitative vs. Quantitative CRP testing
Qualitative CRP
Reports as Negative or Positive. Threshold is typically 0.5 mg/dL. Useful for rapid screening in clinics and emergency settings. Provides no information about severity.
Quantitative CRP
Reports an exact concentration (mg/dL or mg/L). Preferred in hospital settings for monitoring disease progression and treatment response over time. Far more clinically informative.
In most hospital laboratories, quantitative CRP measured by turbidimetric immunoassay (TIA) is the standard. Hs-CRP, measured with even greater precision, is used separately for cardiovascular risk assessment.
3. How the test works: turbidimetric immunoassay (TIA)
Most clinical laboratories use TIA to measure CRP. In this method, anti-CRP antibodies in the reagent bind to CRP in the patient’s serum, forming immune complexes that increase the turbidity (cloudiness) of the solution. A spectrophotometer measures the degree of light scatter or absorbance, and the instrument calculates the CRP concentration from a calibration curve.
TIA is fast, highly reproducible, and fully automated — ideal for high-volume laboratory workflows.
4. Normal reference ranges
The table below reflects widely accepted clinical reference ranges. Always interpret results in the context of your specific laboratory’s reported reference interval.
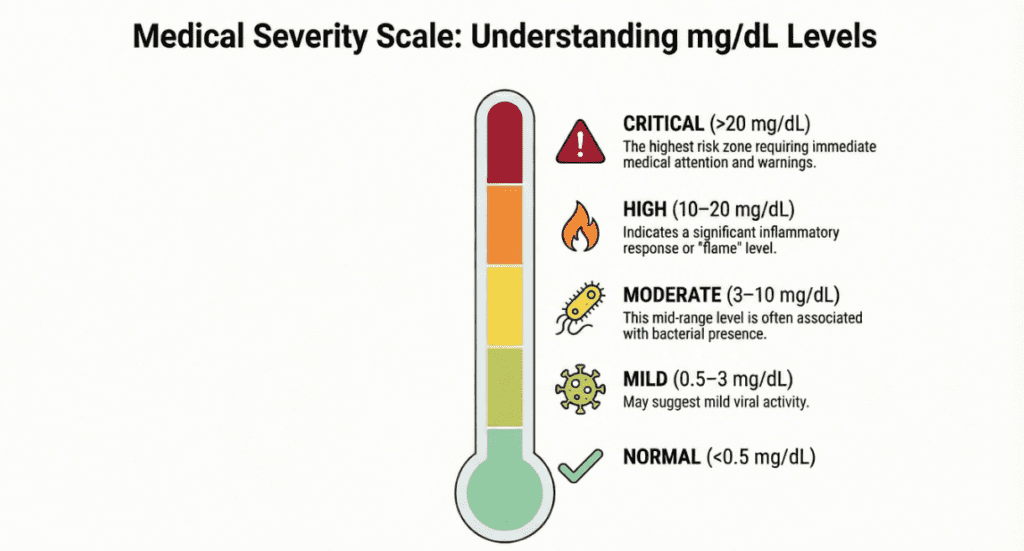
| Level | CRP Range | Unit | Clinical Significance |
|---|---|---|---|
| Normal | < 0.5 | mg/dL | No clinically significant inflammation |
| Mildly elevated | 0.5 – 3.0 | mg/dL | Likely viral infection, mild inflammation |
| Moderate | 3.0 – 10.0 | mg/dL | Bacterial infection possible; autoimmune activity |
| High | 10.0 – 20.0 | mg/dL | Strongly suggests bacterial infection or acute systemic inflammation |
| Very high | > 20.0 – 30.0+ | mg/dL | Severe sepsis, necrotizing fasciitis, critical illness |
* Reference ranges may vary by laboratory. Results must always be interpreted alongside clinical findings.
5. Clinical interpretation
Elevated CRP — what it may indicate
- Bacterial infections: Pneumonia, urinary tract infections, cholecystitis, sepsis
- Autoimmune diseases: Rheumatoid arthritis, systemic lupus erythematosus (in active phase), vasculitis
- Post-surgical or traumatic inflammation: Normal elevation expected after major surgery; persistently high levels suggest complications
- Malignancy: Especially in advanced-stage cancers with paraneoplastic inflammation
- Inflammatory bowel disease: Crohn’s disease tends to elevate CRP more than ulcerative colitis
- Acute pancreatitis: CRP > 15 mg/dL at 48 hours is associated with severe disease
Falling CRP — a good sign, but interpret carefully
- Rapid decrease within 24–48 hours generally signals effective antibiotic or anti-inflammatory treatment
- Serial measurements are more informative than a single value
- A persistent or rising CRP despite treatment should prompt reassessment
Low or normal CRP despite suspected infection
- Viral infections (influenza, RSV, adenovirus) typically cause little to no CRP elevation
- Immunosuppressed patients (those on corticosteroids, chemotherapy, or immunosuppressants) may not mount a normal CRP response
- Early-stage bacterial infections may not yet have elevated CRP
6. Precautions and limitations
Important: A CRP result — high or low — should never be interpreted in isolation. It is a non-specific marker. Always correlate with clinical presentation, patient history, and other laboratory data.
- Medications: Corticosteroids, NSAIDs, and statins can suppress CRP. Failure to account for current medications may lead to underestimation of inflammation.
- Heterophile antibody interference: Rare but documented. May cause falsely elevated or decreased CRP results. Clinically discordant results warrant repeat testing or alternative method confirmation.
- Hook effect: At extremely high CRP concentrations, turbidimetric assays may paradoxically underreport — consider dilution if clinical context is inconsistent.
- Obesity and metabolic syndrome: Chronically mildly elevated CRP is common and does not necessarily indicate active infection.
- Pregnancy: CRP is typically higher in the third trimester; use caution interpreting mild elevations.
- Not a surrogate for procalcitonin: For distinguishing bacterial sepsis from other causes, procalcitonin may offer superior specificity in certain clinical contexts.
7. Specialist’s perspective
From a laboratory medicine standpoint, CRP remains one of the most cost-effective and time-sensitive inflammatory markers available. Its value lies not in a single number but in trends over time. A CRP that rises from 2 mg/dL to 18 mg/dL over 24 hours in a post-operative patient is a red flag demanding immediate clinical attention — even if the absolute value might seem modest in a sepsis context. Conversely, a CRP falling from 22 mg/dL to 8 mg/dL over 48 hours in a patient receiving antibiotics is strong evidence of treatment efficacy. Always pair CRP with clinical assessment, white cell count, differential, and — where appropriate — procalcitonin for the most complete picture of the inflammatory state.
Laboratory Medicine Specialist, MD.phD.
Board-certified specialist in Laboratory Medicine with clinical expertise in immunoassay diagnostics, acute-phase reactants, and infection biomarkers. Committed to translating complex laboratory data into clear, actionable clinical guidance.
What is Serum Amyloid A (SAA) Test? – MedLab Insight
Some images in this post were generated using AI.
References
- Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest. 2003;111(12):1805–1812. doi:10.1172/JCI18921
- Sproston NR, Ashworth JJ. Role of C-reactive protein at sites of inflammation and infection. Front Immunol. 2018;9:754.
- UpToDate. Acute phase reactants. Wolters Kluwer. Accessed April 2026.
- Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl J Med. 1999;340(6):448–454.
- Mayo Clinic Laboratories. C-Reactive Protein, Serum — Test Reference. mayocliniclabs.com. Accessed April 2026.
- National Institutes of Health (NIH). MedlinePlus. C-reactive protein (CRP) test. medlineplus.gov. Accessed April 2026.
- https://pubmed.ncbi.nlm.nih.gov/9971870