
[MD.phD.] “Left Shift” in Blood Tests
Understanding “Left Shift” in Blood Tests: A Laboratory Medicine Specialist’s Guide
Written by a Laboratory Medicine Specialist, MD.phD.
Introduction
If you have ever received a CBC (complete blood count) report and noticed the phrase “left shift,” you may have wondered what it means — and whether it signals something serious. As a Laboratory Medicine Specialist, I encounter this finding regularly, and its interpretation requires careful attention to context. In brief, a left shift means that immature granulocytes — cells that normally remain confined to the bone marrow — have appeared in the peripheral blood circulation. This can reflect a normal stress response, a severe infection, or — less commonly — a bone marrow disorder. This article explains what left shift is, why it occurs, how to interpret it clinically, and when it demands urgent attention.
What Is “Left Shift”?
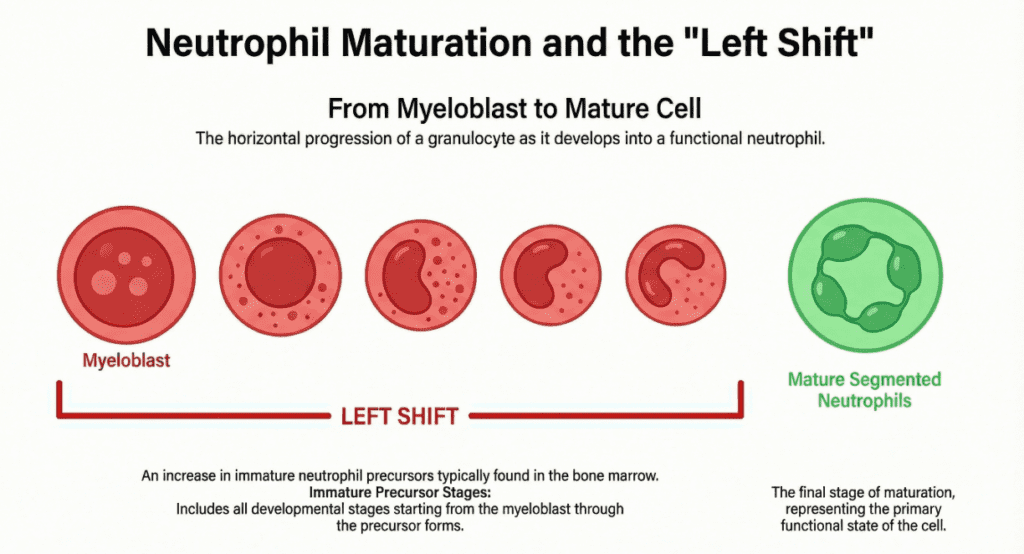
The term “left shift” originates from older manual differential counters, where immature cell types were physically listed on the left side of the counting form. Today, it remains the standard clinical shorthand for an increase in immature granulocytes — particularly band neutrophils, metamyelocytes, and myelocytes — in the peripheral blood smear (PBS).
Under normal conditions, granulocytes mature through a strict sequence within the bone marrow (myeloblast → promyelocyte → myelocyte → metamyelocyte → band → segmented neutrophil) before being released into the bloodstream as mature, fully functional cells. In a healthy adult, fewer than 5% of circulating neutrophils are band forms, and earlier precursors are virtually absent.
A left shift is reported when this orderly release breaks down: the bone marrow dispatches immature forms prematurely, and they appear in counts that exceed normal thresholds.
Why Does Left Shift Occur?
Several distinct mechanisms can produce a left shift:
Increased peripheral demand. In severe infection or inflammation, neutrophils are consumed rapidly in the tissues. The bone marrow responds by accelerating granulopoiesis and releasing immature cells from its storage pool to compensate for the deficit.
Bone marrow hyperstimulation. Elevated levels of colony-stimulating factors (G-CSF, GM-CSF) — whether endogenous or administered therapeutically — drive accelerated proliferation and early release of immature granulocytes.
Marrow reserve depletion. In overwhelming sepsis or severe systemic illness, the marrow’s mature neutrophil reserve becomes exhausted, leaving only immature forms to send out. This scenario — neutropenia combined with left shift — is a particularly ominous finding.
Physiologic or transient causes. Strenuous exercise, post-surgical stress, acute hemorrhage, and vaccination can all produce a transient mild left shift without underlying pathology.
Normal Reference Ranges
The table in the clinical summary widget above provides standard reference values. As a general guide:
| Category | Band Neutrophil % | Interpretation |
|---|---|---|
| Healthy adults | 0–5% | Normal |
| Adults (borderline) | 6–10% | Monitor clinically |
| Adults (significant) | >10% | Investigate further |
| Neonates / infants | Up to 10–15% | Age-adjusted normal |
Reference ranges vary between laboratories and analyzer platforms. Always interpret results in the context of your institution’s reference intervals and the patient’s clinical picture.
Clinical Interpretation
Increased (significant left shift)
A meaningful left shift — especially when combined with the following features — should prompt active clinical evaluation:
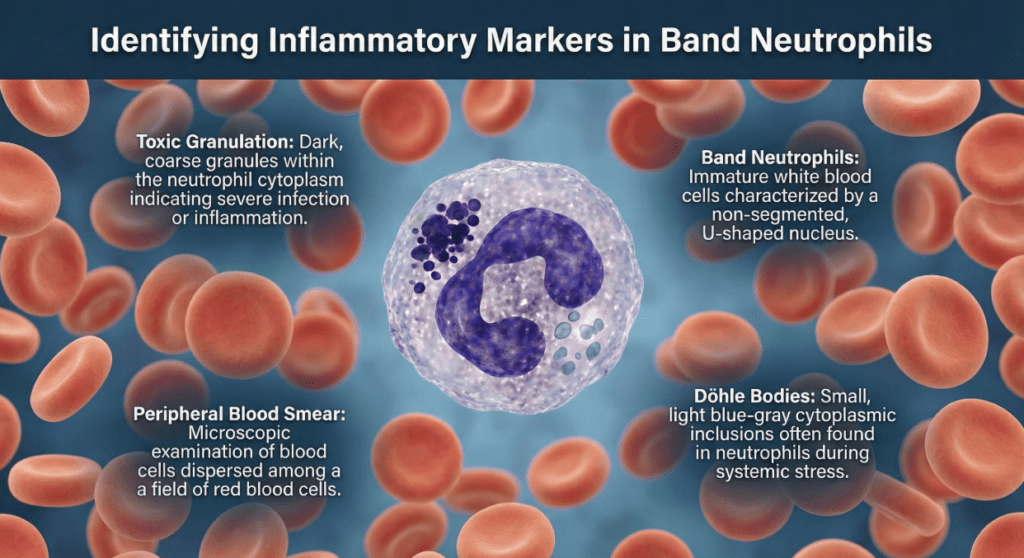
- Elevated WBC + elevated bands + toxic changes on PBS: The combination of left shift with toxic granulation, Döhle bodies, or cytoplasmic vacuolation in neutrophils is a high-specificity marker for acute bacterial infection and systemic inflammatory response.
- Elevated bands with myelocytes or metamyelocytes: Precursor-level left shift suggests an even more vigorous bone marrow response, sometimes seen in severe sepsis, leukemoid reactions, or early leukemia.
- Leukemoid reaction: A WBC >50,000/µL with marked left shift may mimic leukemia but arises from a severe benign trigger (TB, severe infection, hemolysis). Bone marrow evaluation and the leukocyte alkaline phosphatase (LAP) score help differentiate.
- Chronic myeloid leukemia (CML): A persistent left shift with marked basophilia and a full spectrum of myeloid precursors should raise suspicion for CML; BCR-ABL testing is indicated.
Decreased (neutropenia + left shift)
This pairing demands immediate attention. When absolute neutrophil count is low but immature forms are present, it most often reflects one of two dangerous scenarios: the bone marrow has depleted its mature reserve in response to overwhelming sepsis, or marrow production is critically impaired (aplastic anemia, chemotherapy effect, marrow infiltration). In either case, the risk of life-threatening infection is markedly elevated.
Precautions and Limitations
Several important caveats govern the interpretation of left shift:
Automated analyzers have limits. Modern hematology analyzers flag abnormal differential distributions and generate bands-equivalent estimates, but they cannot reliably identify and classify all immature granulocyte subtypes. A manual PBS review by a trained laboratory professional remains essential when a left shift is flagged or suspected.
Single results are not diagnoses. A lone finding of “mild left shift” on one occasion, particularly in a child, a post-operative patient, or someone who exercised vigorously before the draw, is rarely pathological in isolation. Serial testing and trend analysis are far more informative than a single data point.
Pediatric age adjustments matter. Neonates and infants physiologically circulate a higher proportion of band forms. Using adult reference intervals in this population leads to significant over-reporting of left shift.
Medications and growth factors. Exogenous G-CSF administration (used in oncology and neutropenia management) reliably produces a pronounced left shift as a therapeutic effect; this should not be misinterpreted as infection.
Left shift is a finding, not a diagnosis. It must be contextualized with inflammatory markers (CRP, procalcitonin, ferritin), clinical history, culture results, and imaging before any conclusion is drawn.
A Specialist’s Perspective
In my experience, the most clinically actionable pattern is the triad of leukocytosis + significant left shift + toxic changes on PBS. When all three are present in a febrile patient, the probability of acute bacterial infection is high enough to warrant empirical antibiotic therapy while cultures are pending — even before a definitive organism is identified.
Conversely, an isolated mild band increase (6–9%) with no toxic changes, no fever, and a clear precipitant (recent surgery, marathon run, recent vaccine) rarely warrants escalation beyond a follow-up CBC in 48–72 hours.
The key takeaway is proportionality: the significance of left shift scales with the clinical context, the absolute magnitude of the shift, and what else is present on the smear. The lab result is a signal; the diagnosis belongs to the full clinical picture.
Author Profile
This article was authored by a board-certified specialist in Laboratory Medicine and Clinical Pathology with experience in hematology interpretation, quality assurance, and clinical consultation. The information provided is intended for educational purposes and does not constitute individual medical advice. Always consult your physician or laboratory medicine specialist for interpretation of your specific results.
Body Fluid Analysis: Interpretation Guide – MedLab Insight
Some images in this post were generated using AI.
References
- Tefferi, A., & Hanson, C. A. (2020). Hematologic disorders: Approach to the patient. In UpToDate. Retrieved from https://www.uptodate.com
- Wollner, C., & Bhatt, D. L. (2021). Leukocytosis. In Merck Manual Professional Edition. https://www.merckmanuals.com
- Riley, R. S., Ben-Ezra, J. M., & Massey, D. (2015). The peripheral blood smear. In Henry’s Clinical Diagnosis and Management by Laboratory Methods (23rd ed.). Elsevier.
- Hoffman, R., et al. (2018). Hematology: Basic Principles and Practice (7th ed.). Elsevier.
- National Institutes of Health / MedlinePlus. (2023). CBC with differential. https://medlineplus.gov/lab-tests/complete-blood-count-cbc/