
[MD.PhD.] GGT Test (Gamma-Glutamyl Transferase) (26)
Understanding GGT (Gamma-Glutamyl Transferase): A Laboratory Medicine Specialist’s Complete Guide
Authored by a Board-Certified Laboratory Medicine Specialist (MD.PhD.), this guide covers everything clinicians and informed patients need to know about the GGT blood test — from its enzymatic basis to nuanced clinical interpretation in liver, biliary, and metabolic disease.
Quick summary: GGT (Gamma-Glutamyl Transferase) is a liver enzyme routinely measured as part of a liver function panel. It is particularly valuable for identifying cholestasis, alcohol-related liver damage, and drug-induced liver injury. Significantly elevated GGT alongside alkaline phosphatase (ALP) strongly suggests hepatobiliary disease, while a normal GGT with elevated ALP points toward bone pathology — a critical clinical distinction.
What is GGT & why is it ordered?
Gamma-Glutamyl Transferase (GGT) is a membrane-bound enzyme found primarily in the liver, biliary epithelium, kidneys, pancreas, and prostate. Its physiological role is to catalyze the transfer of gamma-glutamyl groups from glutathione and other peptides to acceptor molecules — a key step in amino acid transport and glutathione metabolism across cell membranes.
When hepatocytes or biliary epithelial cells are stressed, damaged, or exposed to enzyme-inducing agents, GGT leaks into the bloodstream in measurable quantities. This makes it a sensitive — though not highly specific — early marker of hepatobiliary dysfunction. Clinicians order this test in the following scenarios:
- Suspected liver or biliary tract disease: Including cholestasis, biliary obstruction, hepatitis, and cirrhosis.
- ALP source differentiation: When ALP is elevated, GGT helps determine whether the elevation originates from the liver or from bone.
- Alcohol-related liver assessment: GGT is among the most sensitive serum markers of chronic alcohol use and alcohol-induced liver injury.
- Drug-induced liver injury monitoring: Particularly with anticonvulsants (phenytoin, carbamazepine), rifampin, steroids, and other microsomal enzyme inducers.
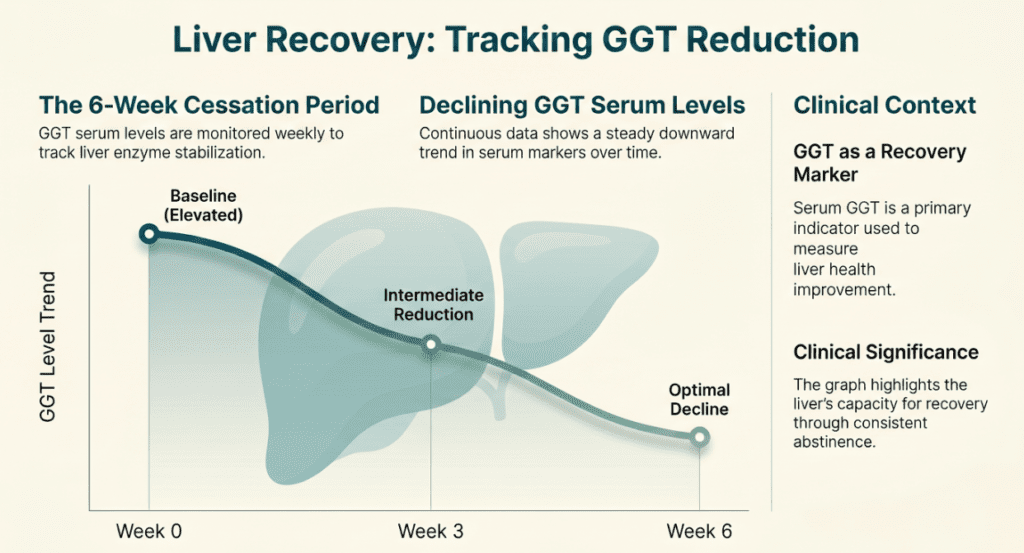
- Treatment response monitoring: Tracking recovery of GGT toward baseline after alcohol cessation, drug withdrawal, or treatment of fatty liver disease.
Measurement principle — enzymatic assay
GGT activity is measured using a standardized colorimetric enzymatic assay, widely implemented on fully automated chemistry analyzers in accredited laboratories worldwide.
- Substrate reaction: The reagent contains a synthetic gamma-glutamyl donor — most commonly γ-glutamyl-p-nitroanilide — along with an acceptor peptide such as glycylglycine.
- GGT catalysis: GGT in the patient’s serum transfers the gamma-glutamyl group to glycylglycine, releasing p-nitroaniline as the chromogenic product.
- Photometric detection: The rate of p-nitroaniline formation is measured by absorbance at 405 nm. The rate of absorbance increase is directly proportional to GGT enzymatic activity in the sample.
This method is highly reproducible, linear across a broad dynamic range, and is the international standard for GGT quantification in clinical laboratories.
Normal reference ranges
| Category | Normal range | Unit / notes |
|---|---|---|
| Adult males | 10 – 70 | U/L |
| Adult females | 6 – 40 | U/L |
| Elderly (≥65 years) | Slightly higher | U/L (age-related drift) |
| Late pregnancy | Often lower than baseline | U/L (physiological) |
| Newborns / infants | Substantially higher | U/L (age-dependent, separate neonatal ranges apply) |
* Reference ranges may vary by laboratory instrument, reagent manufacturer, and patient population. Always interpret results against your institution’s established reference interval. Males have higher GGT in part because the enzyme is also expressed in prostate tissue.
Clinical interpretation
Elevated GGT — causes & mechanisms
- Cholestasis & biliary obstruction: Gallstones, cholangitis, primary sclerosing cholangitis, or tumor-related bile duct compression all impair bile flow. The resulting biliary back-pressure induces upregulation of GGT expression in bile duct epithelium. GGT rises in parallel with ALP and bilirubin.
- Alcoholic liver disease: Chronic alcohol consumption is one of the most potent inducers of hepatic GGT synthesis. Even moderate alcohol use can elevate GGT; in chronic heavy drinkers, levels can reach 5–10× the upper limit of normal. GGT typically normalizes within 2–6 weeks of abstinence, making it a useful sobriety biomarker.
- Non-alcoholic fatty liver disease (NAFLD / NASH): GGT is frequently elevated in patients with metabolic syndrome, obesity, insulin resistance, and type 2 diabetes — conditions that drive hepatic lipid accumulation and oxidative stress.
- Viral & drug-induced hepatitis: Hepatocellular damage from any cause — including acute viral hepatitis, autoimmune hepatitis, and toxic liver injury — elevates GGT, typically in conjunction with marked ALT and AST rises.
- Enzyme-inducing medications: A class of drugs known as microsomal enzyme inducers — including phenytoin, carbamazepine, rifampin, phenobarbital, and chronic alcohol — upregulate hepatic cytochrome P450 enzymes and concurrently induce GGT. This effect can occur without true liver cell damage.
- Pancreatic disease: Acute and chronic pancreatitis, or pancreatic neoplasms causing biliary compression, can produce secondary GGT elevation through biliary involvement.
- Hyperthyroidism & cardiac failure: Secondary liver congestion in right heart failure and hyperthyroid states have been associated with mild GGT elevation.
Decreased GGT — clinical context
GGT decreases are generally not clinically significant in isolation. However, the following states may be associated with lower-than-expected values:
- Hypothyroidism: Reduced metabolic activity and decreased enzyme synthesis can lower circulating GGT.
- Late pregnancy (third trimester): Physiological hemodilution and hormonal changes typically reduce serum GGT, which should not be misinterpreted as a liver abnormality.
- Patients on hemodialysis: Complex metabolic alterations associated with end-stage renal disease and dialysis have been associated with lower GGT values.
The most important clinical use: ALP source differentiation
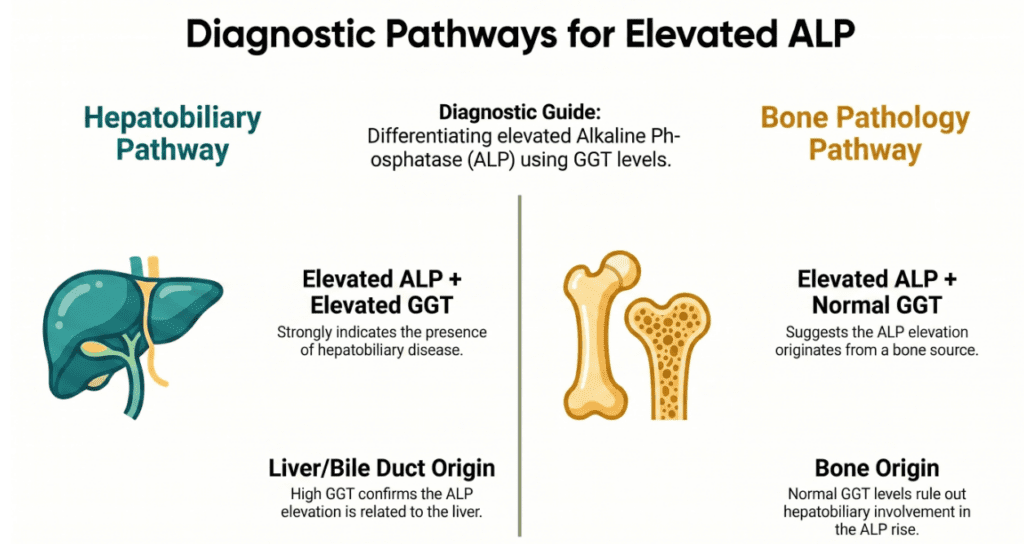
In clinical practice, GGT’s single most valuable application is resolving the ambiguity of an elevated ALP. Because ALP is present in both liver and bone, an elevated ALP alone cannot confirm hepatobiliary disease. GGT resolves this elegantly:
| Pattern | GGT status | Most likely source |
|---|---|---|
| ALP elevated | GGT also elevated | Liver / biliary origin — cholestasis, hepatitis, drug effect |
| ALP elevated | GGT normal | Bone origin — Paget’s disease, fracture, bone metastasis, vitamin D deficiency |
| GGT elevated alone | — | Often enzyme induction (alcohol, drugs), early NAFLD, metabolic risk |
Practical rule: GGT does not rise in bone disease. If ALP is elevated but GGT is normal, the liver is not the culprit — redirect your workup toward skeletal pathology.
Precautions & limitations
Sensitivity vs. specificity
GGT is highly sensitive for hepatobiliary injury but has low specificity. It rises with alcohol, obesity, drugs, and even smoking — do not interpret in isolation.
Medication effects
Anticonvulsants, rifampin, steroids, and oral contraceptives can elevate GGT via enzyme induction without true liver damage.
Lifestyle factors
Smoking, obesity, and even moderate social alcohol use raise GGT. A mildly elevated GGT in an otherwise healthy, asymptomatic patient warrants clinical context — not immediate alarm.
Pregnancy
GGT falls in late pregnancy due to dilution and hormonal effects. Normal pregnant ranges differ from standard adult ranges.
- Always interpret GGT in conjunction with ALT, AST, ALP, and bilirubin — never as a standalone diagnostic marker.
- An AST:ALT ratio greater than 2, combined with a disproportionately elevated GGT, is a classic pattern for alcoholic liver disease.
- GGT has been investigated as a marker of cardiovascular risk and oxidative stress (via glutathione metabolism), but it is not currently validated as a cardiovascular biomarker in clinical guidelines.
- A single mildly elevated GGT result should never be used for self-diagnosis. Repeat testing, clinical correlation, and specialist evaluation are essential before reaching any diagnostic conclusion.
Specialist’s perspective & conclusion
Over years of reviewing liver function panels, the question I encounter most often from clinicians is: “The ALP is elevated — is this liver or bone?” GGT answers that question almost instantly and with remarkable reliability. Its co-elevation with ALP is one of the most practical binary decision points in clinical chemistry.
That said, I consistently caution against over-interpreting isolated GGT elevations. A GGT of 55 U/L in a 45-year-old man who drinks two glasses of wine nightly, has a BMI of 28, and takes carbamazepine may simply reflect the sum of multiple enzyme-inducing exposures — not occult cirrhosis. Context is everything.
For clinicians monitoring patients through alcohol cessation programs, GGT is a particularly gratifying marker: it responds quickly and consistently to abstinence, often normalizing within four to six weeks. Watching GGT trend downward is both diagnostically validating and motivationally useful for patients.
Key takeaway: GGT is sensitive, responsive, and clinically versatile — but it is a supporting actor, not the lead. Paired with ALP, AST/ALT, and bilirubin, it transforms a simple enzyme panel into a powerful hepatobiliary diagnostic toolkit.
Written by a Board-Certified Laboratory Medicine Specialist
Specialist in Laboratory Medicine & Clinical Pathology. Expertise in clinical chemistry, hepatobiliary biomarkers, and laboratory quality management. This content is for educational purposes only and does not constitute individualized medical advice.
[MD.PhD.] Urinary Urea Nitrogen (UUN) (26) – MedLab Insight
[MD.PhD.] High-Sensitivity Troponin T (hs-TnT) Test (26) – MedLab Insight
Some images are generated by AI.
References
- Lott, J. A., & Turner, K. (1975). Evaluation of Trinder’s glucose oxidase method for measuring glucose in serum and urine. Clinical Chemistry, 21(12), 1754–1760. [Historical enzymatic colorimetry foundation]
- Teschke, R. (2018). Alcoholic liver disease: Alcohol metabolism, cascade of molecular mechanisms, cellular targets, and clinical aspects. Biomedicines, 6(4), 106. https://doi.org/10.3390/biomedicines6040106
- Whitfield, J. B. (2001). Gamma glutamyl transferase. Critical Reviews in Clinical Laboratory Sciences, 38(4), 263–355.
- Dufour, D. R., Lott, J. A., Nolte, F. S., et al. (2000). Diagnosis and monitoring of hepatic injury. Clinical Chemistry, 46(12), 2027–2049.
- Mayo Clinic Laboratories. (2024). Gamma-glutamyltransferase (GGT), serum. https://www.mayocliniclabs.com
- Pratt, D. S., & Kaplan, M. M. (2023). Evaluation of liver disease in adults: Laboratory assessment. UpToDate. Wolters Kluwer.
- European Association for the Study of the Liver (EASL). (2023). EASL clinical practice guidelines on non-invasive tests for evaluation of liver disease severity and prognosis. Journal of Hepatology, 77(6), 1547–1583.
- EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis – 2021 update – PubMed