
[MD.PhD.] Anti-TPO and Anti-Thyroglobulin Antibodies (2026)
Anti-TPO and Anti-Thyroglobulin Antibodies: A Specialist’s Guide to Thyroid Autoimmunity Testing
Anti-TPO antibody and Anti-thyroglobulin antibody (TG Ab) are the two cornerstones of thyroid autoimmunity testing — essential for diagnosing Hashimoto’s thyroiditis, supporting a diagnosis of Graves’ disease, and predicting future thyroid dysfunction. This article, authored by a Laboratory Medicine Specialist, explains what each antibody means, how to interpret results, what can cause false positives, and how these tests integrate into broader thyroid evaluation.
Laboratory Medicine Specialist, MD.PhD. Board-certified in Clinical Pathology & Laboratory Medicine
1 What are anti-TPO and anti-TG antibodies?
These two tests detect autoantibodies — immune proteins mistakenly produced against the body’s own thyroid tissue. Together, they provide a window into the underlying autoimmune process that drives the majority of thyroid dysfunction worldwide.
Anti-TPO antibody
Targets thyroid peroxidase, the key enzyme that catalyzes thyroid hormone synthesis. The most sensitive autoantibody for autoimmune thyroid disease — elevated in the vast majority of Hashimoto’s cases.
Anti-TG antibody (TG Ab)
Targets thyroglobulin, the protein scaffold inside thyroid follicles from which T3 and T4 are cleaved. Less sensitive than Anti-TPO alone, but adds diagnostic value when used together.
Historical note
Anti-TPO Ab was formerly known as antimicrosomal antibody (MS Ab) or thyroid microsomal antibody (TM Ab). The current standardized name — Anti-TPO Ab — reflects its specific molecular target. Older laboratory reports may still use the legacy terminology.
Clinical indications — when does a doctor order these tests?
- Suspected Hashimoto’s thyroiditis (autoimmune hypothyroidism)
- Supporting diagnosis of Graves’ disease (autoimmune hyperthyroidism)
- Unexplained thyroid function abnormalities (TSH, Free T4 out of range without clear cause)
- Postpartum thyroiditis or recurrent pregnancy loss workup
- Screening high-risk individuals (family history of thyroid disease, other autoimmune conditions)
- Monitoring risk of future hypothyroidism in antibody-positive euthyroid patients
- Interpreting thyroglobulin (TG) measurements in thyroid cancer surveillance (TG Ab causes interference)
2 Measurement method: ECLIA
Most accredited laboratories measure both antibodies using Electrochemiluminescence Immunoassay (ECLIA) — the current gold standard for thyroid autoantibody quantification.
High sensitivity and specificity
Detects low-level antibody positivity that older methods may miss
Fully automated
Reduces inter-run variability; results reproducible across runs
Minimal sample volume
A small serum aliquot is sufficient — convenient for panels
Quantitative output
Reports continuous IU/mL values, enabling trend tracking over time
3 Normal reference ranges
The thresholds below reflect widely used cut-offs based on ECLIA platforms (e.g., Roche Elecsys). Cut-off values differ between assay manufacturers — always refer to your laboratory’s printed reference interval on the report.
| Antibody | Reference range | Unit | Interpretation |
|---|---|---|---|
| Anti-TPO Ab | < 34.0 | IU/mL | Negative / Normal |
| TG Ab (Anti-TG) | < 115.0 | IU/mL | Negative / Normal |
| Anti-TPO Ab — borderline | 34 – 60 | IU/mL | Repeat + clinical correlation |
| Anti-TPO Ab — clearly elevated | > 60 | IU/mL | Likely autoimmune thyroid disease |
| TG Ab — low-titer positive | 115 – 300 | IU/mL | Can occur in healthy individuals |
| TG Ab — significantly elevated | > 300 | IU/mL | Strongly suggests autoimmune thyroid disease |
Laboratory note
Reference ranges vary by reagent manufacturer, assay platform, and patient population. The cut-offs above are commonly cited but not universal. Always use the reference interval printed on your laboratory’s report. Values from different laboratories using different assays cannot be directly compared.
4 Clinical interpretation
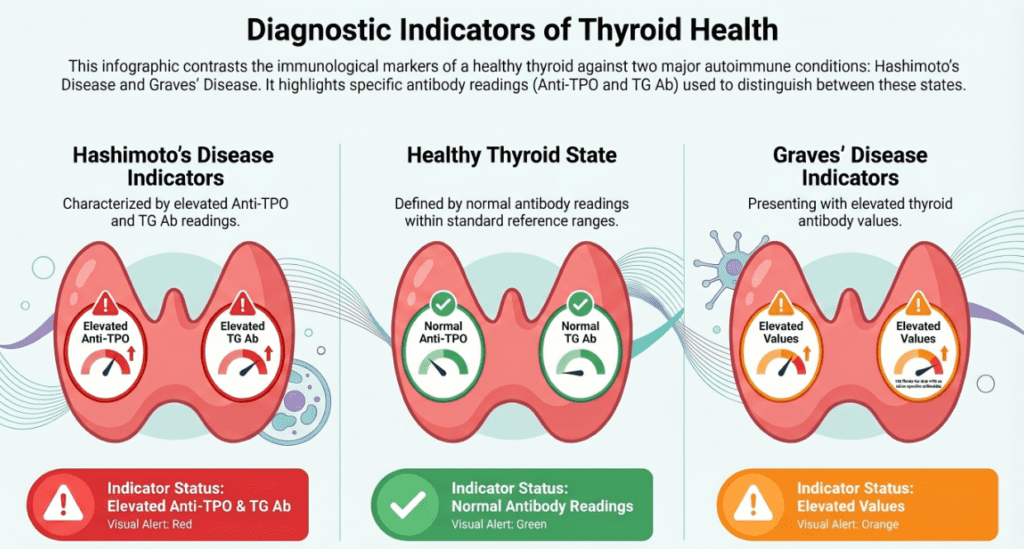
Elevated anti-TPO antibody — associated conditions
Anti-TPO Ab: the most sensitive thyroid autoantibody
Anti-TPO Ab is positive in 90–95% of Hashimoto’s thyroiditis cases and 60–80% of Graves’ disease cases, making it the single most informative antibody in the thyroid autoimmunity panel.
- Hashimoto’s thyroiditis (chronic autoimmune thyroiditis) — the primary diagnostic marker; levels often markedly elevated (hundreds to thousands IU/mL)
- Graves’ disease — positive in 60–80%; TRAb (TSH receptor antibody) is the more specific test for Graves’, but Anti-TPO confirms the autoimmune backdrop
- Postpartum thyroiditis — elevated prenatally predicts risk; fluctuates during the postpartum period
- Silent/painless thyroiditis
- Euthyroid autoimmunity — antibody-positive individuals with normal TSH have a ~2–4% annual progression rate to overt hypothyroidism
- Other autoimmune diseases — type 1 diabetes, rheumatoid arthritis, systemic lupus erythematosus, celiac disease (concurrent autoimmunity)
Elevated TG Ab — associated conditions
- Hashimoto’s thyroiditis — positive in ~60–80% of cases; less sensitive than Anti-TPO but adds complementary value
- Graves’ disease — frequently co-elevated with Anti-TPO
- Thyroid cancer (differentiated) — critical to identify before thyroglobulin (TG) monitoring, as TG Ab interferes with TG immunoassays and causes falsely low readings
- Low-titer positivity in healthy individuals — low levels (115–300 IU/mL) can occasionally occur without clinical disease, particularly in older women
Key clinical pearl — TG Ab and thyroid cancer surveillance
In patients treated for differentiated thyroid cancer, TG Ab acts as an interferent in serum TG immunoassays, causing underestimation of TG — a critical tumor marker. TG Ab must always be measured alongside TG, and a rising TG Ab titer may itself signal disease recurrence even when TG appears low.
Negative / low antibody levels — what does it mean?
- Autoimmune thyroid disease is less likely — but cannot be completely excluded
- A seronegative form of Hashimoto’s exists (antibody-negative autoimmune thyroiditis confirmed on histology in ~5–10% of cases)
- May represent an early or quiescent phase of disease before antibody levels rise
- Suggests non-autoimmune causes of thyroid dysfunction (e.g., iodine deficiency, subacute De Quervain’s thyroiditis, drug-induced thyroid disease)
Important limitation
A negative antibody result does not rule out autoimmune thyroid disease. Clinical judgment, TSH, Free T4, and thyroid ultrasound findings must all be considered together before excluding the diagnosis.
5 Precautions and limitations
| Factor | Effect on result | Clinical action |
|---|---|---|
| Female sex | 2–3× higher prevalence of positive antibodies than males | Use sex- and age-appropriate clinical context |
| Advanced age | Low-titer positivity more common without disease | Correlate with TSH; low-titer alone may not warrant treatment |
| Pregnancy | Anti-TPO levels may fall in second/third trimester due to immune suppression, then rebound postpartum | Test in first trimester for risk stratification |
| Immunosuppressants | May reduce antibody titers artificially | Document medications when interpreting |
| ARNI / immune checkpoint inhibitors | Checkpoint inhibitors (cancer immunotherapy) can trigger de novo thyroid autoimmunity | Screen before and during therapy |
| Iodine excess | High iodine intake may trigger or exacerbate autoimmune thyroiditis | Assess dietary/supplement iodine history |
| Assay platform differences | Values not interchangeable across manufacturers | Always use the same laboratory for serial monitoring |
- Antibody titers do not reliably correlate with disease severity or symptom burden — a very high titer does not necessarily mean worse disease
- These tests are primarily diagnostic tools, not reliable treatment response monitors; TSH and Free T4 remain the primary markers for monitoring thyroid function
- Always interpret alongside TSH, Free T4, and thyroid ultrasound — no single test is sufficient in isolation
- Do not use these results for self-diagnosis. A positive antibody requires clinical evaluation by a qualified physician
Self-diagnosis warning
Thyroid antibody results require interpretation by a qualified clinician in the context of your symptoms, thyroid function tests (TSH, Free T4), and imaging findings. An isolated positive antibody — particularly at low titer — does not mean you have thyroid disease or require treatment.
6 Specialist’s perspective and conclusion
In my experience managing thyroid laboratory panels, one of the most common interpretive errors I encounter is over-reliance on a positive antibody result as a standalone diagnosis. A patient with Anti-TPO Ab at 50 IU/mL and a normal TSH does not necessarily have symptomatic Hashimoto’s thyroiditis — they may be in a pre-clinical autoimmune phase that warrants monitoring, not treatment.
Conversely, I frequently see negative or borderline antibody results used to dismiss an autoimmune diagnosis in patients with classic symptoms and an echogenic, heterogeneous thyroid on ultrasound. In those cases, seronegative autoimmune thyroiditis must still be considered.
Three practical rules I apply in daily laboratory consultation:
- Order both antibodies together — Anti-TPO alone misses ~15–20% of Hashimoto’s cases that are TG Ab-positive only; the combination maximizes sensitivity.
- Always order TG Ab before any thyroglobulin measurement in a thyroid cancer follow-up context — discovering TG Ab interference after the fact can delay critical clinical decisions.
- Serial monitoring of antibody titers is rarely necessary — once positive and the diagnosis established, TSH and Free T4 are the management markers. Repeat antibody testing every few years is reasonable only if the clinical picture changes significantly.
Key takeaways
1. Anti-TPO Ab is the most sensitive single antibody for autoimmune thyroid disease — positive in ~90–95% of Hashimoto’s cases. 2. TG Ab adds complementary value and is essential in thyroid cancer surveillance. 3. Negative antibodies do not exclude autoimmune thyroid disease. 4. Always interpret with TSH, Free T4, and clinical findings — never in isolation. 5. Antibody titer does not correlate with symptom severity or treatment response.
About the author
This article was authored by a board-certified Laboratory Medicine Specialist (MD.PhD.) with expertise in clinical pathology, thyroid biomarkers, and immunoassay interpretation. The author has extensive experience translating complex laboratory results into actionable clinical guidance, and all content is reviewed against current international guidelines from the American Thyroid Association (ATA), European Thyroid Association (ETA), and IFCC.
[MD.PhD.] Understanding CA72-4 – MedLab Insight
[MD.phD.] CYFRA 21-1 Tumor Marker – MedLab Insight
References
- Jonklaas, J., et al. (2014). Guidelines for the treatment of hypothyroidism. Thyroid, 24(12), 1670–1751. https://doi.org/10.1089/thy.2014.0028
- Ross, D. S., et al. (2016). 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid, 26(10), 1343–1421. https://doi.org/10.1089/thy.2016.0229
- Kahaly, G. J., et al. (2018). 2018 European Thyroid Association guideline for the management of Graves’ hyperthyroidism. European Thyroid Journal, 7(4), 167–186. https://doi.org/10.1159/000490384
- Pearce, E. N., Farwell, A. P., & Braverman, L. E. (2003). Thyroiditis. New England Journal of Medicine, 348(26), 2646–2655. https://doi.org/10.1056/NEJMra021194
- Spencer, C. A. (2013). Clinical utility and pitfalls of sensitive TSH assays. Clinical Chemistry, 34(8), 1777–1783. https://doi.org/10.1093/clinchem/34.8.1777
- Haugen, B. R., et al. (2016). 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer. Thyroid, 26(1), 1–133. https://doi.org/10.1089/thy.2015.0020
- UpToDate. (2025). Diagnosis of Hashimoto’s thyroiditis (autoimmune thyroiditis). Wolters Kluwer. https://www.uptodate.com
- Mayo Clinic Laboratories. (2025). Anti-thyroid peroxidase antibody (anti-TPO) test interpretation. https://www.mayocliniclabs.com
- TPO – Overview: Thyroperoxidase Antibodies, Serum