
[MD.phD.] CYFRA 21-1 Tumor Marker
CYFRA 21-1 Tumor Marker: A Specialist’s Guide to Lung Cancer Diagnosis and Monitoring
By a Laboratory Medicine Specialist, MD.phD.
CYFRA 21-1 (Cytokeratin 19 Fragment) is a serum tumor marker with particular clinical value in non-small cell lung cancer (NSCLC), especially squamous cell carcinoma. This article — written by a board-certified Laboratory Medicine Specialist — explains what CYFRA 21-1 measures, how to interpret elevated levels across different lung cancer stages, what non-malignant conditions can raise the result, and why this marker is most powerful as a monitoring tool rather than a standalone diagnostic test.
What is CYFRA 21-1 and why is it ordered?
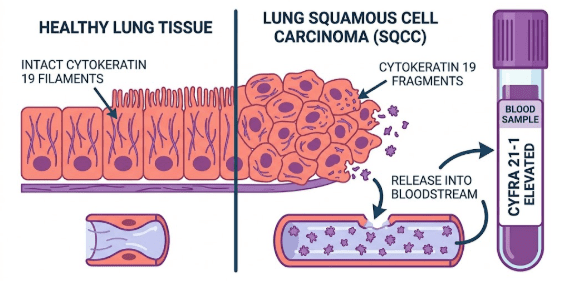
CYFRA 21-1 stands for Cytokeratin 19 Fragment. Cytokeratin 19 is an intermediate filament protein that forms part of the cytoskeletal scaffolding of epithelial cells — the cell type that lines the airways, alveoli, and much of the respiratory tract. Under normal physiological turnover, tiny amounts of this protein are shed into the bloodstream. When epithelial cells undergo accelerated destruction, necrosis, or malignant transformation, significantly larger fragments are released, raising the measurable serum concentration.
Clinicians order this test in the following contexts:
- Supportive diagnosis and staging of suspected or confirmed NSCLC
- Monitoring treatment response after surgery, chemotherapy, or radiotherapy
- Surveillance for recurrence in patients with previously treated lung cancer
- Prognostic stratification alongside imaging and pathology findings
CYFRA 21-1 is not used as a population-level screening test for lung cancer; its sensitivity in early-stage disease is insufficient for that purpose.
Normal reference ranges
| Population / Condition | Normal Range | Unit |
|---|---|---|
| Healthy adults (general) | < 3.3 | ng/mL |
| Non-smokers | < 3.3 | ng/mL |
| Smokers (mild elevation possible) | Typically < 3.3 – 3.5 | ng/mL |
| Patients with benign lung disease | May reach 3.3 – 5.0 (context-dependent) | ng/mL |
| Clinically significant elevation (lung cancer context) | > 3.3 (interpret with imaging and history) | ng/mL |
⚠ Reference ranges vary between laboratories and assay platforms. Always interpret results against your institution’s validated reference interval. Values cited here reflect commonly reported thresholds in the published literature (ECLIA / CMIA platforms).
CYFRA 21-1 across lung cancer stages
A defining clinical feature of CYFRA 21-1 is its strong correlation with tumor burden and disease stage. The higher the stage, the greater the likelihood — and magnitude — of elevation:
Stage I. Often normal
Tumor burden is low. Sensitivity is limited; a normal result does not exclude early lung cancer.
Stage II – III. Moderate elevation
Regional lymph node involvement and locoregional invasion drive measurable increases.
Stage IV. Markedly elevated
Distant metastases, extensive necrosis, and high tumor load produce the highest values. Strongly associated with poor prognosis.
Post-treatment
Serial trend matters
A falling level signals response; rising levels after nadir suggest recurrence or progression.
Clinical interpretation: elevated CYFRA 21-1
Lung cancer — the primary concern
Among all lung cancer histotypes, CYFRA 21-1 demonstrates the strongest association with:
- Squamous cell carcinoma (SCC) — highest sensitivity among NSCLC subtypes; markedly elevated values are common even at stage II–III. This histotype causes extensive epithelial destruction, releasing large quantities of cytokeratin fragments.
- Adenocarcinoma — can also elevate CYFRA 21-1, though typically to a lesser degree than SCC at comparable stages. CEA is often a more sensitive complementary marker in adenocarcinoma.
- Large cell carcinoma — moderate elevation, less consistent than SCC.
- Small cell lung cancer (SCLC) — CYFRA 21-1 is less specific here; NSE and ProGRP are preferred markers for SCLC.
Non-malignant causes of elevated CYFRA 21-1
CYFRA 21-1 is not cancer-specific. The following benign conditions must be considered before attributing an elevated result to malignancy:
- Liver disease (hepatitis, cirrhosis) — impaired hepatic clearance raises baseline levels
- Chronic kidney disease / renal failure — reduced renal excretion of cytokeratin fragments
- Pulmonary infections, pneumonia, lung abscess
- Active pulmonary tuberculosis
- Benign pleural disease (pleural effusion, empyema)
- Smoking — a mild, chronic elevation may be present in heavy smokers without malignancy
- Other epithelial-origin malignancies (bladder, cervical, head and neck cancers) — less commonly, but relevant in patients with known co-existing cancers
Low or normal CYFRA 21-1
A result within the reference range does not exclude lung cancer. In early-stage NSCLC (stage I), the majority of patients will have normal or near-normal CYFRA 21-1 levels. Normal results in the correct clinical context should prompt continued evaluation through CT imaging, bronchoscopy, or biopsy — not reassurance that cancer is absent.
CYFRA 21-1 as a treatment monitoring tool
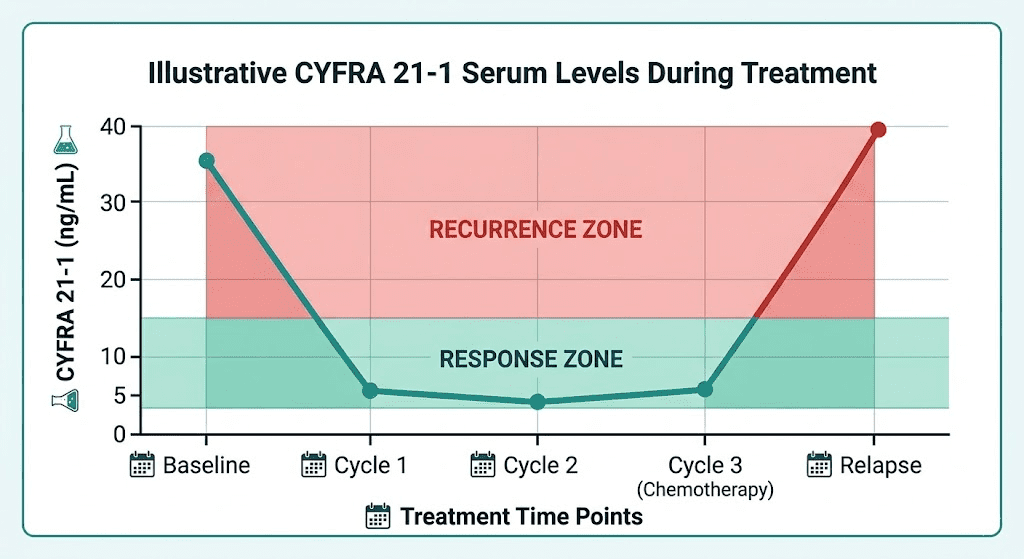
This is arguably where CYFRA 21-1 delivers its greatest clinical value. Serial measurements taken at defined intervals after treatment initiation provide objective biochemical evidence of tumor response:
📉 Falling levels after treatment
Indicates a favorable response to chemotherapy, targeted therapy, immunotherapy, or radiotherapy. A rapid decline in the first 1–2 cycles correlates with improved progression-free survival in multiple studies.
📈 Rising levels after initial response (nadir)
A sustained increase ≥25% above the nadir on two consecutive measurements should prompt imaging evaluation for disease progression or recurrence — even in the absence of new symptoms.
⚡ Persistently elevated despite treatment
May indicate primary treatment resistance or residual disease. Consider histological re-evaluation, repeat staging CT, or PET-CT in this scenario.
Precautions and limitations
CYFRA 21-1 cannot be used as a stand-alone screening or diagnostic test for lung cancer. Imaging confirmation and histopathological diagnosis are mandatory before clinical decisions are made.
Renal impairment and hepatic disease can cause false elevations independent of tumor activity. Always review creatinine and liver function tests alongside CYFRA 21-1 in affected patients.
No established cut-off reliably distinguishes malignant from benign causes at levels between 3.3–10 ng/mL — this “grey zone” requires careful clinical correlation.
Smoking alone can cause a mild chronic elevation. Adjust interpretation in heavy long-term smokers without a new clinical change.
For optimal monitoring, use the same assay platform consistently across serial measurements. Inter-platform variability can produce apparent changes in level that do not reflect true biological change.
CYFRA 21-1 should be interpreted as part of a panel — alongside CEA (adenocarcinoma), NSE / ProGRP (SCLC), and SCC antigen (squamous carcinoma) — for the most informative clinical picture.
Specialist’s perspective
In my experience reviewing tumor marker panels across lung cancer patients, one of the most common clinical misunderstandings is treating CYFRA 21-1 as either a “diagnostic” or a “screening” tool. It is neither. Its true power lies in longitudinal tracking.
A patient with stage III squamous cell lung cancer whose CYFRA 21-1 drops from 38 ng/mL to 6 ng/mL after two cycles of platinum-based doublet chemotherapy is giving the oncology team a biochemical signal of response that imaging alone — which lags by weeks — may not yet confirm. Conversely, a quiet but consistent upward trend from 4.1 → 5.8 → 8.2 ng/mL across three months in a patient considered to be in remission should never be dismissed: in my clinical observation, such a pattern frequently precedes radiologically detectable recurrence by 4–8 weeks.
The key takeaway: order CYFRA 21-1 with a serial monitoring strategy in mind, document the baseline before treatment, and always integrate the trend — not just the absolute value — into the clinical narrative alongside CT, PET, and pathology.
Laboratory Medicine Specialist, MD.phD.
Board-certified specialist in clinical and laboratory medicine with expertise in tumor marker diagnostics, hematology, and pre-analytical quality management. This article is intended for educational purposes and does not constitute individual medical advice. All clinical decisions should involve a qualified physician and multidisciplinary team.
Anti-CCP Antibody Test – MedLab Insight
CH50 (Total Complement Activity) Test – MedLab Insight
Some medical images generated by AI.
References
- Plebani M, Cervellin G, Lippi G. Tumor markers in lung cancer: state-of-the-art and perspectives. Advances in Clinical Chemistry. 2012;56:1–36. doi:10.1016/B978-0-12-394317-0.00013-7
- Schneider J, Philipp M, Velcovsky HG, Morr H, Katz N. Pro-gastrin-releasing peptide (ProGRP), neuron-specific enolase (NSE), carcinoembryonic antigen (CEA) and cytokeratin 19-fragments (CYFRA 21-1) in patients with lung cancer in comparison to other lung diseases. Anticancer Research. 2003;23(2A):885–893.
- Grunnet M, Sorensen JB. Carcinoembryonic antigen (CEA) as tumor marker in lung cancer. Lung Cancer. 2012;76(2):138–143. doi:10.1016/j.lungcan.2011.11.012
- Molina R, et al. CYFRA 21-1 in non-small cell lung cancer: comparison with CEA, CA 125, SCC and NSE serum tumor markers. Anticancer Research. 1999;19(4A):2537–2547.
- Ferrigno D, Buccheri G, Giordano C. Neuron-specific enolase is an effective tumour marker in non-small cell lung carcinoma. Lung Cancer. 2003;41(3):311–320. doi:10.1016/S0169-5002(03)00273-7
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Non-Small Cell Lung Cancer. Version 2025. Available at: https://www.nccn.org
- Marrades RM, et al. Compartmental analysis of CYFRA 21-1 in patients with exudative pleural effusions. Respiration. 2000;67(4):431–437.
- https://pubmed.ncbi.nlm.nih.gov/12928122