[MD.PhD.] HbA1c Testing & Hemoglobin Variants
HbA1c Testing & Hemoglobin Variants: A Laboratory Specialist’s Complete Guide to Accurate Interpretation
Why your glycated hemoglobin result may be misleading — and what to do about it.
Laboratory Medicine Specialist, MD.phD.
HbA1c (glycated hemoglobin) is the gold-standard test for diagnosing and monitoring diabetes, reflecting average blood glucose over the past 2–3 months. However, genetic hemoglobin variants — such as HbS, HbC, HbE, and thalassemia-related variants — can critically distort HbA1c readings, depending on the measurement method used. This guide explains how variants affect results, which patients are most at risk, and what alternative markers clinicians should use when HbA1c becomes unreliable.
What Is HbA1c and Why Does It Matter?
HbA1c — or glycated hemoglobin — measures the proportion of hemoglobin in red blood cells that has bonded with glucose through a non-enzymatic process called glycation. Because red blood cells have a lifespan of approximately 120 days, this test provides a reliable snapshot of an individual’s mean blood glucose concentration over the preceding 2–3 months.
Two major global bodies govern the standardization of HbA1c measurement:
- IFCC (International Federation of Clinical Chemistry and Laboratory Medicine)
- NGSP (National Glycohemoglobin Standardization Program, USA)
This standardization is what allows HbA1c to be used consistently across laboratories worldwide — making it indispensable for both diabetes diagnosis and long-term management goals.
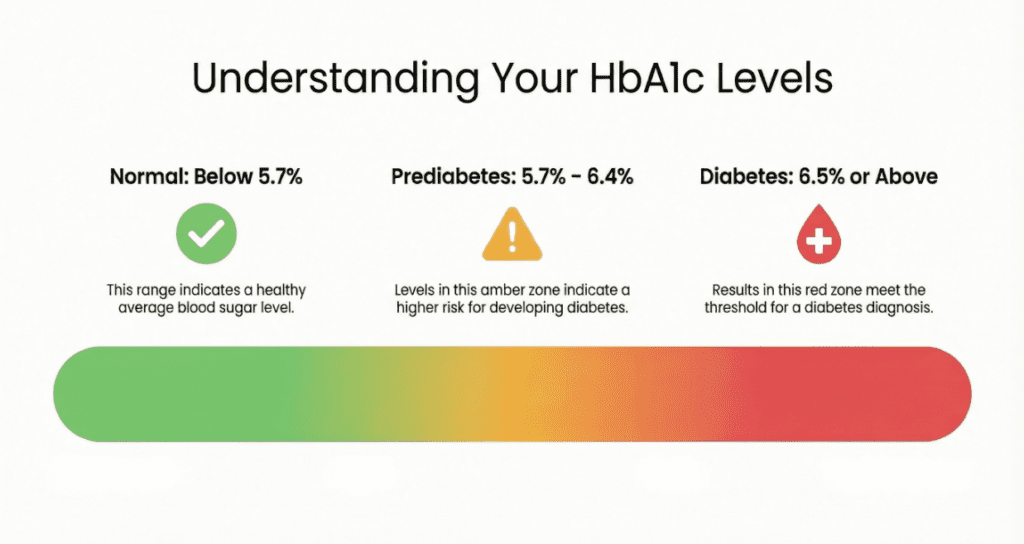
Reference Ranges & Diagnostic Thresholds
| Category | HbA1c (NGSP %) | HbA1c (IFCC mmol/mol) | Clinical Interpretation |
|---|---|---|---|
| Normal (Non-diabetic) | < 5.7% | < 39 mmol/mol | No current risk indication |
| Prediabetes | 5.7 – 6.4% | 39 – 46 mmol/mol | Increased risk; lifestyle intervention advised |
| Diabetes (diagnostic threshold) | ≥ 6.5% | ≥ 48 mmol/mol | Diabetes diagnosis (confirm with repeat test) |
| Well-controlled diabetes (target) | < 7.0% | < 53 mmol/mol | General ADA glycemic target for most adults |
| Suboptimal control | 7.0 – 8.0% | 53 – 64 mmol/mol | Treatment review recommended |
| Poor control / High complication risk | > 8.0% | > 64 mmol/mol | Urgent treatment optimization required |
* Reference ranges may vary slightly by laboratory and clinical guideline (ADA, EASD, WHO). Always interpret in clinical context.
What Are Hemoglobin Variants and Why Are They Problematic?
HbA1c testing is premised on the assumption that a patient carries standard hemoglobin A (HbA). In reality, a significant proportion of the global population carries structural hemoglobin variants — genetically encoded differences in the globin chain amino acid sequence. Common variants include:
- HbS — Associated with sickle cell disease; most prevalent in sub-Saharan Africa, the Caribbean, and the Middle East
- HbC — Primarily found in West African populations
- HbE — Extremely prevalent across Southeast Asia (up to 30–60% carrier rates in some regions)
- Alpha (α) and Beta (β) thalassemia variants — Widespread across the Mediterranean, Middle East, and Asia
- Other rare variants — HbD, HbG, HbJ, and many others
Clinician Note
In South Korea and other East Asian countries, the increasing prevalence of migrant populations from Southeast Asia, the Middle East, and Central Asia means hemoglobin variants are no longer a rare consideration — they are an emerging clinical reality that every laboratory and clinician must address.
How Hemoglobin Variants Distort HbA1c Results
The measurement method used determines how — and how much — a variant will affect the HbA1c result. Understanding this is essential for laboratory interpretation.
HPLC (Ion-Exchange Chromatography)
Most widely used method. Separates hemoglobin fractions by charge. Variants can co-elute with HbA1c, create anomalous peaks, or shift retention times — producing falsely elevated or falsely low results.
Immunoassay
Uses antibodies targeting the N-terminal glycated peptide of the β-chain. If a variant alters this region (e.g., HbS), antibody binding fails — typically causing falsely low HbA1c values or assay failure.
Enzymatic Methods
Generally more resistant to variant interference than HPLC or immunoassay. However, no method is completely immune, and cross-validation remains essential for confirmed variant carriers.
Altered Red Cell Lifespan: An Underappreciated Mechanism
Beyond assay interference, many hemoglobin variants directly shorten or lengthen red cell lifespan. Because HbA1c accumulates throughout the red cell’s life, a patient with hemolytic anemia (shorter lifespan) will show falsely low HbA1c — even with poor glycemic control — while conditions causing longer cell survival may give falsely elevated values entirely unrelated to blood glucose.
Clinical Interpretation: High vs. Low HbA1c in the Context of Variants
Falsely Elevated HbA1c
- Variant co-eluting with the HbA1c fraction on HPLC
- Iron deficiency anemia (increased RBC age distribution → more glycation time)
- Vitamin B12 or folate deficiency
- Splenectomy (prolonged RBC survival)
- Renal failure with erythropoietin deficiency (older cell population)
Falsely Decreased HbA1c
- Hemolytic anemia (shortened RBC lifespan — common with HbS, HbC, HbE homozygotes)
- Post-transfusion state (dilution of patient’s glycated hemoglobin)
- Pregnancy (physiological hemodilution, increased RBC turnover)
- Erythropoietin or iron therapy (accelerated new RBC production)
- Antibody interference in immunoassay methods
Real-World Clinical Consequences of HbA1c Interference
Risk 1 — Misdiagnosis of Diabetes
A falsely elevated HbA1c ≥ 6.5% in a normoglycemic patient carrying a hemoglobin variant can lead to an incorrect diabetes diagnosis, triggering unnecessary medication, patient anxiety, and insurance or employment consequences.
Risk 2 — Inappropriate Treatment Intensification
If a treated diabetic patient’s HbA1c appears elevated due to variant interference, clinicians may escalate insulin doses or add pharmacotherapy — causing unnecessary hypoglycemic risk in a patient whose actual glycemic control is adequate.
Risk 3 — Missed Poor Control
Conversely, a falsely low HbA1c in a patient with hemolysis may create a false sense of therapeutic success. Actual hyperglycemia goes undetected, and complication risk accumulates silently.
Precautions, Limitations & Confounding Factors
Beyond hemoglobin variants, several other conditions and clinical factors can compromise HbA1c reliability:
- Pregnancy: Physiological hemodilution and increased red cell turnover lower HbA1c independent of glycemia; fasting plasma glucose or continuous glucose monitoring (CGM) is preferred for gestational diabetes diagnosis.
- Chronic kidney disease (CKD): Erythropoietin deficiency and anemia alter RBC populations; HbA1c may underestimate true glycemic burden.
- Recent blood transfusion: Donor RBCs (non-glycated) dilute the patient’s own HbA1c for up to 3 months.
- High-dose vitamin C or E supplementation: May inhibit in vitro glycation in stored blood samples.
- Aspirin in high doses: May cause acetylation of hemoglobin, potentially interfering with some assay methods.
Important Disclaimer
HbA1c is a population-validated screening and monitoring tool. A single result should never be used in isolation for diagnosis or treatment decisions. All results must be interpreted within the full clinical picture, including symptoms, concurrent medications, and comorbidities.
What to Do When HbA1c May Be Unreliable
Step 1 — Suspect Interference When You See:
- Unusual peaks or abnormal chromatogram on HPLC printout
- HbA1c result inconsistent with point-of-care blood glucose or CGM data
- Sudden unexplained change in HbA1c not consistent with clinical history
- Patient from a high-prevalence variant population (Southeast Asian, South Asian, Middle Eastern, African, or Mediterranean ancestry)
Step 2 — Use an Alternative Glycemic Biomarker
Glycated Albumin (GA)
Reflects ~2–3 week glucose average; preferred alternative when variants confirmed
Fructosamine
Similar 2–3 week window; useful when albumin turnover is normal
CGM (Continuous Glucose Monitoring)
Real-time glucose data; unaffected by hemoglobin structure
Fasting Plasma Glucose
Direct glucose measurement; useful for diagnosis in variant carriers
Step 3 — Confirm the Variant
When variant interference is strongly suspected, hemoglobin electrophoresis or high-resolution HPLC hemoglobin characterization can definitively identify the variant type. HPLC laboratories should also routinely flag and report any anomalous chromatogram patterns to referring clinicians.
Specialist’s Perspective & Key Takeaways
In my laboratory practice, I encounter cases of variant-related HbA1c discordance more frequently than many clinicians expect. The critical habit is always to compare HbA1c with available self-monitoring blood glucose logs or CGM data. When these don’t correlate, never simply repeat the same HbA1c — investigate the cause. A reliable diagnosis and appropriate treatment depend on reliable data. When the data may not be reliable, we must have the intellectual honesty to acknowledge that, and pivot to validated alternatives. Glycated albumin, in particular, has proven itself to be an excellent, underutilized tool in variant carriers.
— Laboratory Medicine Specialist, MD.phD.
The key takeaways for every clinician and lab professional:
- HbA1c is the cornerstone of diabetes management — but it assumes normal hemoglobin.
- Hemoglobin variants (HbS, HbC, HbE, thalassemia) are globally common and growing in frequency due to migration.
- Both measurement method and red cell lifespan can cause false high or false low HbA1c values.
- Always cross-check HbA1c with direct blood glucose or CGM data in high-risk patients.
- Glycated albumin is the best practical alternative when HbA1c is unreliable.
- Laboratories must report HPLC chromatogram anomalies — they are a critical clinical signal.
Laboratory Medicine Specialist, MD.phD.
Board-Certified Specialist · Clinical Chemistry & Hematology
A board-certified Laboratory Medicine physician with clinical and research expertise in clinical chemistry, hematology, and diagnostic accuracy. This content is intended for educational purposes for clinicians and informed patients, and does not constitute personal medical advice.
When HBsAg and Anti-HBs Are Both Positive – MedLab Insight
EDTA-Dependent Pseudothrombocytopenia – MedLab Insight
References
- American Diabetes Association. (2024). Standards of Medical Care in Diabetes — 2024. Diabetes Care, 47(Suppl 1), S1–S321. https://doi.org/10.2337/dc24-SINT
- National Institute of Diabetes and Digestive and Kidney Diseases. (2023). The A1C Test & Diabetes. National Institutes of Health. https://www.niddk.nih.gov/health-information/diagnostic-tests/a1c-test
- Little, R. R., & Roberts, W. L. (2009). A review of variant hemoglobins interfering with hemoglobin A1c measurement. Journal of Diabetes Science and Technology, 3(3), 446–451. https://doi.org/10.1177/193229680900300307
- Gallagher, E. J., Le Roith, D., & Bloomgarden, Z. (2009). Review of hemoglobin A1c in the management of diabetes. Journal of Diabetes, 1(1), 9–17. https://doi.org/10.1111/j.1753-0407.2009.00009.x
- Bry, L., Chen, P. C., & Sacks, D. B. (2001). Effects of hemoglobin variants and chemically modified derivatives on assays for glycohemoglobin. Clinical Chemistry, 47(2), 153–163.
- International Federation of Clinical Chemistry (IFCC). (2023). Reference system for measurement of HbA1c in human blood. https://www.ifcc.org/ifcc-scientific-division/sd-committees/c-mhba1c/
- Saudek, C. D., & Brick, J. C. (2009). The clinical use of hemoglobin A1c. Journal of Diabetes Science and Technology, 3(4), 629–634.
- https://pubmed.ncbi.nlm.nih.gov/11159762