[MD.PhD.] Hb Levels and Symptoms (2026)
Low Hemoglobin, No Symptoms? A Specialist Explains Why Hb Levels and Anemia Symptoms Don’t Always Match
Hematology, Laboratory Medicine, April 13, 2026
As a Laboratory Medicine Specialist, one of the most common questions I receive is: “How can a patient with a hemoglobin of 4 g/dL still be walking and talking?” The short answer is that anemia symptoms depend far more on how fast hemoglobin drops and who the patient is than on the absolute number itself. This article explains the physiological mechanisms behind this disconnect, defines the reference ranges clinicians use, and describes what factors must be considered alongside any Hb value.
What is hemoglobin and why does it matter?
Hemoglobin (Hb) is the iron-containing protein packed inside red blood cells. Its primary role is to bind oxygen in the lungs and deliver it to every tissue in the body. When hemoglobin falls below the normal threshold — a state called anemia — tissues receive less oxygen, and the body may respond with symptoms ranging from mild fatigue to life-threatening cardiovascular collapse.
Clinicians order hemoglobin testing as part of a complete blood count (CBC) for a wide range of indications: routine health screening, evaluation of fatigue or shortness of breath, monitoring of chronic disease, pre-operative assessment, and management of known bleeding or hematologic disorders.
Normal reference ranges for hemoglobin
| Category | Normal range | Unit |
|---|---|---|
| Adult males | 13.0 – 17.0 | g/dL |
| Adult females | 12.0 – 16.0 | g/dL |
| Pregnant women | ≥11.0 (WHO threshold) | g/dL |
| Children (6 months – 5 years) | 11.0 – 14.0 | g/dL |
| Children (6 – 14 years) | 12.0 – 16.0 | g/dL |
| Elderly (≥65 years) | Slightly lower; clinical context required | g/dL |
Reference ranges may vary by laboratory, analyzer, and patient population. Always interpret results in the context of institutional reference intervals.
How hemoglobin levels map to clinical symptoms
| Hb level (g/dL) | WHO severity | Typical symptom pattern* |
|---|---|---|
| 10 – 12 | Mild anemia | Usually asymptomatic; mild exertional fatigue possible |
| 8 – 10 | Moderate anemia | Dyspnea on exertion, easy fatigue, mild palpitations |
| 6 – 8 | Severe anemia | Breathlessness at rest, dizziness, pallor, tachycardia |
| 3 – 5 | Very severe | High-risk; however, chronic cases may surprisingly tolerate this range |
| < 3 | Life-threatening | Myocardial ischemia, syncope, hemodynamic instability |
*This table reflects population-level tendencies. Individual tolerance varies considerably — see section below.
Why symptoms and Hb levels often don’t match
This is where laboratory medicine meets physiology — and where the most clinically important nuance lies.
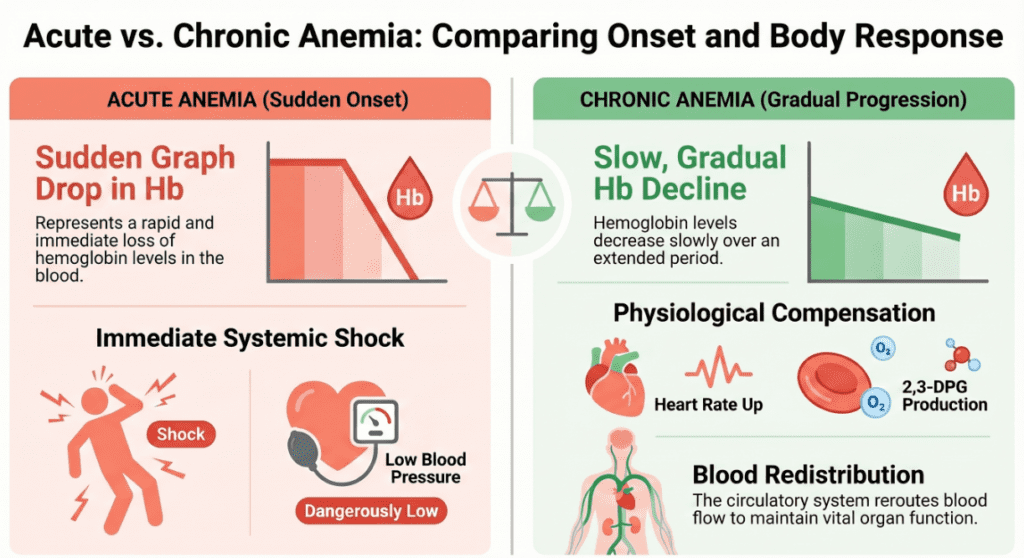
Acute anemia (rapid onset)
- Body has no time to compensate
- Hb of 8 g/dL can cause hypotension or shock
- Classic presentation: dizziness, syncope, rapid heart rate, low blood pressure
- Typical cause: acute hemorrhage, hemolytic crisis
Chronic anemia (slow progression)
- Body activates multiple compensatory mechanisms over weeks to months
- Hb of 4–5 g/dL may cause minimal symptoms
- Patient may walk in unassisted, appear alert, deny major complaints
- Typical cause: iron deficiency, chronic disease, B12/folate deficiency
The four key compensation mechanisms in chronic anemia
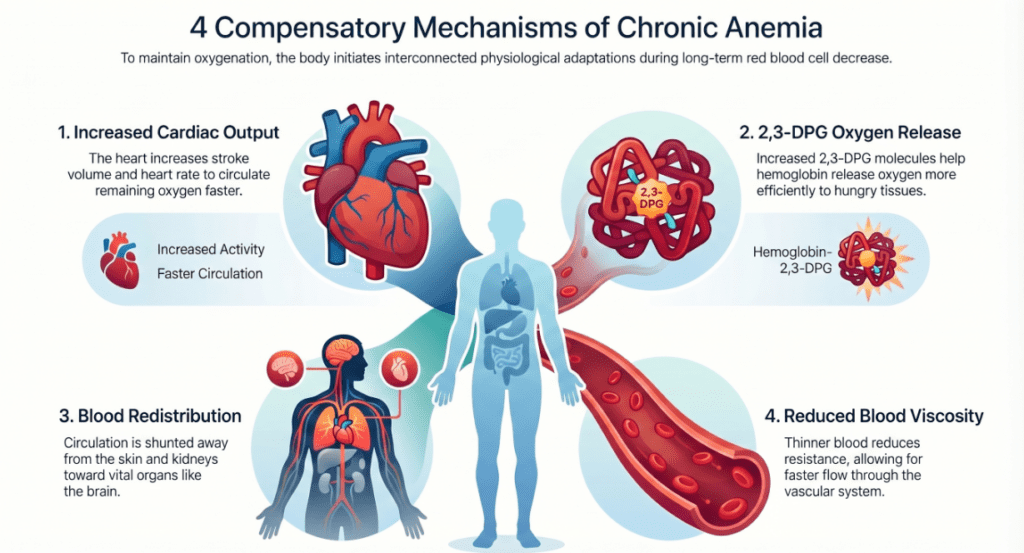
Cardiovascular adaptation
Increased heart rate and stroke volume raise cardiac output, maintaining oxygen delivery despite lower Hb concentration.
2,3-DPG shift
Red cells increase 2,3-diphosphoglycerate (2,3-DPG), shifting the oxygen-hemoglobin dissociation curve rightward — releasing more oxygen to tissues at lower partial pressures.
Blood flow redistribution
Peripheral vasodilation and preferential shunting of blood to the brain, heart, and kidneys help protect vital organs at the expense of skin and muscles.
Reduced blood viscosity
Lower red cell mass decreases blood viscosity, allowing blood to flow more easily through microvasculature — a short-term circulatory advantage, though not a safe long-term state.
Clinical interpretation: what drives individual tolerance?
Factors that worsen tolerance (symptoms appear at higher Hb)
- Heart failure or ischemic heart disease — the heart cannot compensate with increased output
- Chronic obstructive pulmonary disease (COPD) — compromised oxygen loading further limits delivery
- Advanced age — reduced physiological reserve across all organ systems
- High metabolic demand — fever, infection, thyrotoxicosis, or pregnancy increase oxygen requirements
Factors that improve tolerance (symptoms appear at lower Hb)
- Young age and good baseline cardiovascular fitness
- Sedentary lifestyle or low activity level — reduced oxygen demand
- Very gradual onset over months — allows maximal compensation to occur
- Low basal metabolic rate (e.g., elderly patients with limited mobility)
Precautions and clinical limitations
A hemoglobin value in isolation is one of the most easily misinterpreted numbers in laboratory medicine. The Hb level tells you how much oxygen-carrying protein is present — it does not tell you how fast it fell, whether the heart can compensate, or what is causing the anemia in the first place.
Never use a single Hb result to estimate a patient’s clinical risk without also reviewing the rate of decline, vital signs, symptoms, comorbidities, and the clinical context of the draw.
The following factors must always be considered alongside the Hb result:
- Rate of Hb decline (acute vs. chronic onset — this is the single most important modifier)
- Vital signs: heart rate, blood pressure, respiratory rate, oxygen saturation (SpO₂)
- Age and baseline cardiopulmonary function
- Underlying conditions: heart failure, COPD, coronary artery disease
- Evidence of active bleeding or ongoing hemolysis
- Hydration status — hemodilution lowers Hb; dehydration falsely elevates it
- Medications: erythropoiesis-stimulating agents, chemotherapy, anticoagulants
- Nutritional status: iron, B12, folate deficiency
- Pregnancy — physiologic hemodilution lowers Hb without representing true anemia
A specialist’s perspective
In my years of laboratory practice, I have received urgent phone calls about critically low hemoglobin values in patients who were sitting up in bed reading. Every time, the follow-up question from the clinical team is the same: “Is this real?” The answer is almost always yes — the value is accurate — but the clinical impact depends entirely on the story behind the number.
The most dangerous misconception I encounter is the assumption that a “tolerated” low Hb means a safe low Hb. A patient with a chronic Hb of 4 g/dL who appears well is not fine — they are compensating at the absolute limit of physiological reserve. Any additional insult (infection, fluid shift, cardiac stress) can push them into decompensation rapidly. That is why we transfuse based on the clinical trend and trajectory, not just the number on the day.
The key message for both clinicians and patients is this: the Hb value is the starting point of the clinical conversation, not the conclusion. Rate of change, compensatory capacity, and the underlying cause matter as much as — or more than — the absolute number.
Written by a Laboratory Medicine Specialist, MD.PhD.
Board-certified in Clinical Pathology and Laboratory Medicine with over a decade of experience in hematology, clinical chemistry, and diagnostic interpretation. Special interest in bridging laboratory data with bedside clinical decision-making and patient education.
When HBsAg and Anti-HBs Are Both Positive – MedLab Insight
EDTA-Dependent Pseudothrombocytopenia – MedLab Insight
References
- World Health Organization. (2011). Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. WHO/NMH/NHD/MNM/11.1. Geneva: WHO.
- Camaschella, C. (2015). Iron-deficiency anemia. New England Journal of Medicine, 372(19), 1832–1843. https://doi.org/10.1056/NEJMra1401038
- Weiskopf, R. B., et al. (1998). Human cardiovascular and metabolic response to acute, severe isovolemic anemia. JAMA, 279(3), 217–221.
- Carson, J. L., et al. (2016). Red blood cell transfusion: a clinical practice guideline from the AABB. Annals of Internal Medicine, 160(6), 418–430.
- UpToDate. (2025). Diagnostic approach to anemia in adults. Wolters Kluwer. Retrieved from https://www.uptodate.com
- Mayo Clinic Laboratories. (2025). Hemoglobin, blood — test catalog. Retrieved from https://www.mayocliniclabs.com
- Guyton, A. C., & Hall, J. E. (2020). Textbook of Medical Physiology (14th ed., pp. 481–495). Elsevier.
- https://pubmed.ncbi.nlm.nih.gov/22751760