When HBsAg and Anti-HBs Are Both Positive
When HBsAg and Anti-HBs Are Both Positive: A Laboratory Medicine Specialist’s Guide to Interpretation
Introduction
Written by a Laboratory Medicine Specialist, MD
Hepatitis B virus (HBV) serology is among the most frequently ordered panels in routine health screening and liver disease workup worldwide. While most clinicians are comfortable interpreting straightforward positive or negative results, an uncommon yet clinically significant scenario — the simultaneous presence of HBsAg (surface antigen) and Anti-HBs (surface antibody) — can create genuine diagnostic confusion.
This article explains what it means when both HBsAg and Anti-HBs are reactive on the same sample, walks through the three most plausible biological mechanisms, and outlines a practical step-by-step approach to resolving the discordant result. Whether you are a clinician, laboratorian, or an informed patient, this guide will help you interpret this paradoxical finding with confidence.
What Are Hepatitis B Serological Markers and Why Do They Matter?
Hepatitis B serology refers to a panel of blood tests that detect viral proteins (antigens) and the immune system’s response to them (antibodies). Together, these markers allow clinicians to determine whether a patient is currently infected, has recovered, is immune through vaccination, or is in a chronic carrier state.
The standard panel typically includes the following markers:
| Marker | Full Name | Clinical Meaning |
|---|---|---|
| HBsAg | Hepatitis B Surface Antigen | Produced by infected hepatocytes; indicates active infection (acute or chronic) |
| Anti-HBs | Antibody to HBsAg | Appears after recovery or vaccination; confers protective immunity |
| HBeAg | Hepatitis B e-Antigen | Reflects active viral replication and high infectivity |
| Anti-HBe | Antibody to HBeAg | Suggests declining replication; appears during recovery |
| Anti-HBc IgM | IgM Antibody to Core Antigen | Marker of acute or recent infection |
| Anti-HBc Total | Total Antibody to Core Antigen | Indicates past or ongoing infection |
A physician orders this panel to stage hepatitis B infection, guide antiviral therapy decisions, confirm vaccine-induced immunity, and screen blood donors or healthcare workers.
Normal Reference Ranges
⚠️ Reference ranges may vary by laboratory and assay platform. Always interpret results in the context of your institution’s established cutoffs.
| Marker | Negative (Non-Reactive) | Positive (Reactive) | Unit / Cutoff |
|---|---|---|---|
| HBsAg | < 1.0 | ≥ 1.0 | S/CO (signal-to-cutoff ratio) |
| Anti-HBs | < 10 | ≥ 10 | mIU/mL |
| HBeAg | < 1.0 | ≥ 1.0 | S/CO |
| Anti-HBe | Reactive = past replication decline | — | Qualitative |
| Anti-HBc IgM | Negative | Positive | Qualitative |
| Anti-HBc Total | Negative | Positive | Qualitative |
In a typical clinical course: HBsAg becomes positive during active infection → Anti-HBs appears after clearance or vaccination → the two markers are almost never simultaneously reactive under normal circumstances.
Clinical Interpretation: Why Are Both HBsAg and Anti-HBs Positive?
This discordant pattern occurs in approximately 3–5% of chronic HBV patients and should never be dismissed as a laboratory error without investigation. Three main mechanisms have been described.
Mechanism 1 — Mutation in the HBsAg “a” Determinant
The “a” determinant is the primary antigenic loop of HBsAg, located between amino acids 124–147 of the S protein, and is the main target of both vaccine-induced and natural Anti-HBs antibodies.
When point mutations occur in this region — most notably the glycine-to-arginine substitution at position 145 (G145R) — the mutant HBsAg can no longer be fully neutralized by circulating Anti-HBs. As a result:
- Anti-HBs is present (generated against wild-type epitopes)
- Yet mutant HBsAg continues to be detected by the assay
- HBV DNA quantification typically confirms ongoing viral replication
This is clinically important because these escape mutants can infect vaccinated individuals and may evade standard HBsAg immunoassays, occasionally producing false-negative HBsAg results despite active infection.
Mechanism 2 — Non-Specific or Cross-Reactive Antibodies
In some patients, particularly those with autoimmune conditions, hypergammaglobulinemia, or recent blood product transfusions, non-specific antibodies may cross-react with the HBsAg detection reagent, producing a false-positive Anti-HBs signal. In this scenario:
- The patient is genuinely HBsAg-positive (truly infected)
- The Anti-HBs result is a laboratory artifact, not true protective immunity
- Repeat testing using a different assay platform often resolves the discrepancy
Mechanism 3 — Dual Infection with Different HBV Genotypes or Subtypes
HBV is classified into at least 10 genotypes (A through J) and multiple serological subtypes (ayw, adw, adr, etc.). If a patient is co-infected with two antigenically distinct HBV strains:
- Antibodies generated against one subtype’s “a” determinant may not fully neutralize the other
- Both HBsAg (from the incompletely neutralized strain) and Anti-HBs (against the other strain) can coexist
- This scenario, while rare, has been documented in immunocompromised patients and injection drug users
Precautions and Limitations
Several factors can affect the accuracy and interpretation of HBV serology results:
- Assay platform variability: Different manufacturers use distinct antibody clones and cutoff values. A result from one analyzer may not be directly comparable to another.
- Immunosuppression: Patients on chemotherapy, biologics, or post-transplant immunosuppressants may have blunted antibody responses, making serological staging unreliable.
- Window period: In very early acute HBV infection, both HBsAg and Anti-HBs may be transiently negative — only Anti-HBc IgM will be reactive.
- Vaccination history: A history of HBV vaccination producing Anti-HBs ≥ 10 mIU/mL does not rule out subsequent breakthrough infection, especially with escape mutants.
- Single result self-diagnosis: A discordant serological result must never be used for self-diagnosis. Clinical context, liver function tests (AST, ALT), and supplementary molecular testing are essential.
Step-by-Step Approach When Both Markers Are Reactive
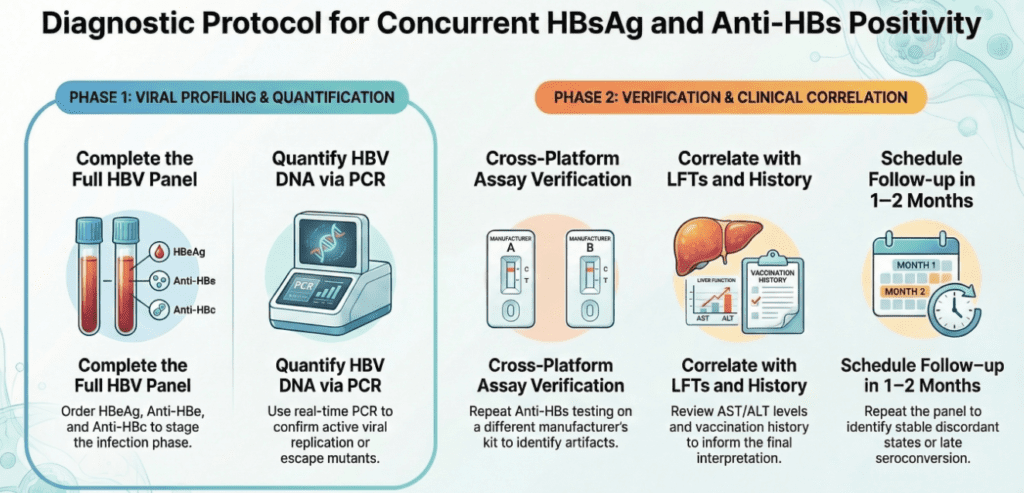
When faced with a simultaneously HBsAg- and Anti-HBs-positive result, the following systematic approach is recommended:
Step 1 — Complete the full HBV panel Order HBeAg, Anti-HBe, Anti-HBc (IgM and total) if not already done. This allows staging of the infection phase and helps distinguish acute from chronic disease.
Step 2 — Quantify HBV DNA HBV DNA by real-time PCR is the gold standard for confirming active viral replication. A detectable or elevated viral load in the presence of Anti-HBs strongly supports an escape mutant or dual-subtype infection.
Step 3 — Repeat on a different assay platform If HBV DNA is undetectable, request a repeat Anti-HBs test using a different manufacturer’s kit. This will identify whether the Anti-HBs signal was platform-specific artifact.
Step 4 — Correlate with liver function tests and clinical history Review AST, ALT, bilirubin, and albumin levels. Incorporate vaccination history, prior HBV infection, current medications, and immune status into the interpretation.
Step 5 — Follow-up testing in 1–2 months A repeat panel after 4–8 weeks can clarify whether the pattern reflects a transitional serological phase (e.g., late seroconversion) or a stable discordant state.
Specialist’s Perspective and Conclusion
From a laboratory medicine standpoint, a simultaneously HBsAg- and Anti-HBs-positive result is one of the most instructive reminders that serological markers must always be interpreted as a panel — not in isolation. In my experience reviewing such cases, the most common cause is an HBsAg escape mutant, followed by non-specific cross-reactivity, and rarely, dual-subtype co-infection.
The key takeaway: do not default to dismissing the result as a lab error. Order HBV DNA quantification immediately. This single additional test will, in the vast majority of cases, determine whether the discordance is clinically meaningful or assay-related.
HBV serology remains one of the most nuanced panels in clinical laboratory medicine. Mastering its interpretation — including paradoxical patterns like this one — is essential for patient safety, appropriate antiviral therapy decisions, and accurate public health surveillance.
Author Profile
This article was written by a board-certified specialist in Laboratory Medicine with clinical expertise in clinical chemistry, immunoassay interpretation, and molecular diagnostics. The author has extensive experience in hepatitis serology interpretation and laboratory quality management in an academic medical center setting.
Understanding the Leptin Blood Test – MedLab Insight
References
- Lok, A. S. F., & McMahon, B. J. (2009). Chronic hepatitis B: Update 2009. Hepatology, 50(3), 661–662. https://doi.org/10.1002/hep.23190
- Tatematsu, K., et al. (2009). A nationwide survey of hepatitis B virus genotypes in Japan. Journal of Medical Virology, 81(8), 1423–1429.
- World Health Organization. (2024). Hepatitis B fact sheet. https://www.who.int/news-room/fact-sheets/detail/hepatitis-b
- Liang, T. J. (2009). Hepatitis B: The virus and disease. Hepatology, 49(S5), S13–S21. https://doi.org/10.1002/hep.22881
- Centers for Disease Control and Prevention. (2023). Interpretation of hepatitis B serologic test results. https://www.cdc.gov/hepatitis/hbv/pdfs/SerologicChartv8.pdf
- Carman, W. F. (1997). The clinical significance of surface antigen variants of hepatitis B virus. Journal of Viral Hepatitis, 4(Suppl 1), 11–20.