
[MD.PhD.] BNP vs NT-proBNP (2026)
BNP and NT-proBNP: A Laboratory Specialist’s Complete Guide to Heart Failure Biomarkers
BNP (B-type natriuretic peptide) and NT-proBNP are the most clinically powerful cardiac biomarkers available for diagnosing acute heart failure, stratifying severity, and guiding prognosis. This guide — written by a Laboratory Medicine Specialist — explains how these two tests work, how to interpret results by age and clinical context, what causes false elevations, and how to choose between them in daily practice.
Laboratory Medicine Specialist, MD.PhD. Board-certified in Clinical Pathology & Laboratory Medicine
1 What Are BNP and NT-proBNP?
Despite its historical name — brain natriuretic peptide — BNP is produced almost exclusively by the ventricular cardiomyocytes of the heart. When the left ventricular wall experiences increased pressure or volume overload, myocardial cells synthesize a precursor called proBNP-108, which is then cleaved by the enzyme corin and neprilysin into two fragments that circulate in blood:
- BNP (amino acids 77–108): the biologically active 32-amino acid peptide that causes natriuresis, diuresis, and vasodilation
- NT-proBNP (amino acids 1–76): the biologically inert N-terminal fragment, but clinically highly useful as a stable marker of cardiac wall stress
In simple terms: the more the heart is under stress, the higher both values climb. Clinicians order these tests whenever a patient presents with dyspnea, edema, or suspected cardiac decompensation.
Clinical Indications — When to Order
Acute dyspnea of uncertain cause (cardiac vs. pulmonary) · Suspected acute or chronic heart failure · Monitoring treatment response in known heart failure · Risk stratification and prognostication in heart failure patients · Ruling out acute heart failure in the emergency setting
2 BNP vs. NT-proBNP: Key Differences
Both fragments originate from the same precursor and both reflect cardiac wall stress — but their biochemical properties differ significantly, which affects how and when each is used clinically.
| Property | BNP | NT-proBNP |
|---|---|---|
| Biological form | Active peptide (natriuretic) | Inactive N-terminal fragment |
| Half-life | ~20 minutes | ~60–120 minutes |
| In-vitro stability | Relatively unstable | Highly stable (can delay processing) |
| Renal clearance | Primarily natriuretic peptide receptors & neutral endopeptidases | Primarily renal clearance — rises markedly in CKD |
| Effect of sacubitril/valsartan | Falsely elevated (neprilysin inhibition reduces BNP clearance) | Not affected |
| Best clinical use | Rapid response marker; acute settings | Diagnosis, staging, long-term monitoring |
| Point-of-care availability | Yes (e.g., Triage® BNP) | Yes (Roche Elecsys®) |
Important Drug Interaction
Patients on sacubitril/valsartan (Entresto®) — an ARNI used in HFrEF — will have artifactually elevated BNP levels due to neprilysin inhibition. Always use NT-proBNP for monitoring in these patients, as NT-proBNP is not affected by sacubitril.
3 Normal Reference Ranges
Reference ranges are age-stratified, particularly for NT-proBNP. Values rise with age due to reduced renal clearance, increasing LV stiffness, and subclinical myocardial changes in older populations. Obesity can lower values. Always use age-appropriate cut-offs and your laboratory’s specific reference intervals.
BNP Reference & Rule-Out / Rule-In Thresholds
| Category | Threshold | Unit | Interpretation |
|---|---|---|---|
| General population (no HF) | < 100 | pg/mL | Normal |
| Rule-out acute HF | < 100 | pg/mL | HF very unlikely (NPV ~96%) |
| Gray zone | 100 – 400 | pg/mL | Indeterminate — consider ADHF, CKD, AF |
| Rule-in acute HF | > 400 | pg/mL | Strongly suggestive of HF |
NT-proBNP Age-Stratified Thresholds (ESC 2021 Guidelines)
| Age Group | Rule-Out Threshold | Rule-In Threshold (Acute HF) | Unit |
|---|---|---|---|
| All ages (chronic HF screening) | < 125 | — | pg/mL |
| < 50 years | < 125 | > 450 | pg/mL |
| 50 – 75 years | < 125 | > 900 | pg/mL |
| > 75 years | < 125 | > 1,800 | pg/mL |
| Obese patients (BMI > 35) | Consider 50% lower thresholds (values attenuated by ~30–40%) | pg/mL | |
Laboratory Note
Reference ranges may vary by assay manufacturer and laboratory. Always interpret results in context of your institution’s validated reference intervals. BNP and NT-proBNP values are not interchangeable — never compare one to thresholds of the other.
4 Clinical Interpretation
🔴 Elevated Levels — Cardiac Causes
- Acute decompensated heart failure (ADHF) — primary indication; values often >2,000 pg/mL in severe cases
- Chronic heart failure (HFrEF & HFpEF) — elevated at baseline, tracks with NYHA class
- Acute myocardial infarction — especially with LV dysfunction
- Cardiac tamponade / constrictive pericarditis
- Hypertrophic cardiomyopathy
- Atrial fibrillation & sustained ventricular arrhythmias
- Severe valvular heart disease (especially aortic stenosis, mitral regurgitation)
🟡 Elevated Levels — Non-Cardiac Causes
This is one of the most clinically important nuances. Significant elevations can occur without heart failure in the following conditions:
| Non-Cardiac Condition | Mechanism | Degree of Elevation |
|---|---|---|
| Chronic kidney disease (CKD) / ESRD | Reduced renal clearance of NT-proBNP | Often markedly elevated |
| Pulmonary embolism (PE) | Acute RV pressure overload | Moderate–high |
| Pulmonary arterial hypertension | Chronic RV strain | Moderate–high |
| Sepsis / critical illness | Cytokine-mediated myocardial injury | Moderate |
| COPD exacerbation | Hypoxia-induced RV stress | Mild–moderate |
| Advanced age (>75 years) | LV stiffening, reduced clearance | Mild–moderate |
| Thyroid dysfunction (hyper- or hypothyroid) | Cardiac metabolic effects | Mild |
| Stroke / subarachnoid hemorrhage | Neurogenic cardiac injury | Mild |
🟢 Low / Normal Levels — The Rule-Out Value
A low BNP or NT-proBNP is arguably the most actionable result in an emergency setting. In a patient with acute dyspnea:
High Negative Predictive Value
BNP < 100 pg/mL or NT-proBNP < 125 pg/mL effectively excludes acute heart failure as the cause of dyspnea, with a negative predictive value (NPV) of approximately 96–98% in the Breathing Not Properly and PRIDE studies. Consider COPD exacerbation, pneumonia, PE, or non-cardiac causes instead.
Very low values may also be seen in:
- Obesity (adipose tissue clears natriuretic peptides and reduces secretion)
- Flash pulmonary edema that has rapidly resolved
- Acute heart failure with early presentation (values may not yet have peaked)
5 Severity, Prognosis & Treatment Monitoring
BNP and NT-proBNP are not merely diagnostic — they are powerful prognostic tools and can serve as therapeutic targets. The relationship between natriuretic peptide levels and clinical outcomes is continuous and graded.
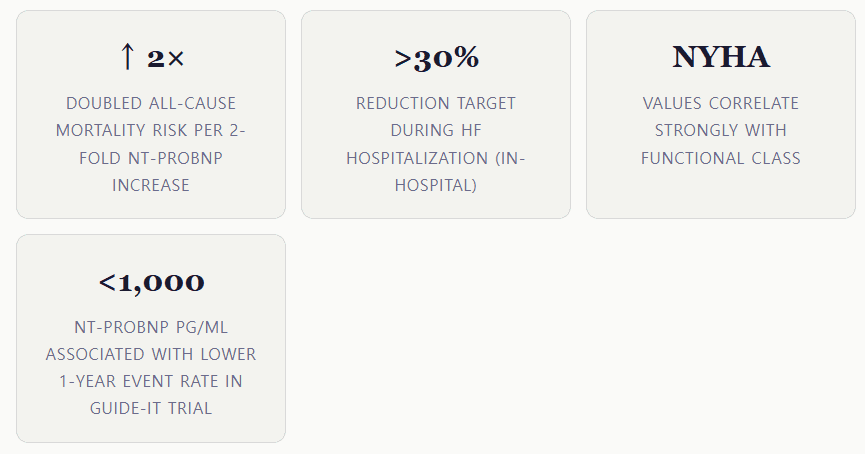
Serial measurements over time are more informative than a single result. A failure to decrease by ≥30% during an acute heart failure hospitalization is associated with increased 30-day readmission and mortality risk (Maisel et al., JACC, 2008).
6 Precautions & Limitations
- BNP and NT-proBNP are not interchangeable. Each assay uses different antibodies; values differ by 2–4-fold. Never compare one test’s result to the other’s thresholds.
- Renal impairment: NT-proBNP rises disproportionately in CKD (GFR <60 mL/min). Use higher age- and GFR-adjusted cut-offs or focus on trend over time.
- Sacubitril/valsartan (ARNIs): Causes spuriously high BNP levels; use NT-proBNP exclusively in these patients.
- Obesity: Both markers are attenuated in obese patients (BMI >35). Consider lower cut-offs or use cautiously.
- Sample handling (BNP): BNP is sensitive to temperature. Samples should be processed promptly; avoid prolonged storage at room temperature.
- Acute vs. chronic HF: In chronic stable HF, a baseline elevated level is expected. Changes from the patient’s own baseline matter more than a single absolute value.
- Not a standalone test: Results must always be interpreted alongside clinical examination, imaging (echocardiography), and the full clinical picture. Do not self-diagnose based on laboratory values.
Self-Diagnosis Warning
BNP and NT-proBNP values require interpretation by a qualified clinician in the context of your complete clinical history, physical examination, and additional investigations. A single elevated or normal value should never be used for self-diagnosis or to alter treatment without medical supervision.
7 Specialist’s Perspective & Conclusion
In my experience as a Laboratory Medicine Specialist, BNP and NT-proBNP remain among the most actionable biomarkers in the entire clinical laboratory repertoire — a rare combination of high negative predictive value for ruling out acute heart failure alongside robust prognostic utility for risk stratification.
The practical decision between the two tests typically comes down to three considerations:
- Medication history: Any patient on sacubitril/valsartan requires NT-proBNP — full stop.
- Renal function: In severe CKD (GFR <30), both markers are elevated; NT-proBNP rises more dramatically, but BNP may offer a slightly less confounded signal in some scenarios.
- Institutional standardization: Hospitals should commit to one assay and train clinicians on its specific thresholds — mixing assays between visits creates dangerous interpretive errors.
One underappreciated clinical pearl: in patients presenting with acute dyspnea where BNP is borderline (100–400 pg/mL), the trajectory often matters more than the absolute number. A BNP rising from 80 to 280 over two hours strongly suggests decompensation even though neither value is dramatically elevated in isolation.
Key Takeaways
1. BNP/NT-proBNP are the gold-standard biomarkers for acute heart failure diagnosis and rule-out. 2. NT-proBNP uses age-stratified cut-offs (450 / 900 / 1,800 pg/mL for <50 / 50–75 / >75 years). 3. Non-cardiac causes — especially CKD — can significantly elevate both markers. 4. For patients on ARNIs, always use NT-proBNP. 5. Serial measurements and trends are more clinically meaningful than isolated values.
About the Author
This article was written by a board-certified Laboratory Medicine Specialist (MD.PhD.) with expertise in clinical pathology, cardiac biomarkers, and laboratory diagnostics. The author has extensive experience in translating complex laboratory data into actionable clinical insights for both specialist and general audiences. All content is reviewed for accuracy against current international guidelines (ESC, ACC/AHA, IFCC).
What is Serum Amyloid A (SAA) Test? – MedLab Insight
[MD.phD.] CRP vs. hs-CRP – MedLab Insight
Some images are generated by AI.
References
- McDonagh, T. A., et al. (2021). 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. European Heart Journal, 42(36), 3599–3726. https://doi.org/10.1093/eurheartj/ehab368
- Maisel, A. S., et al. (2002). Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. New England Journal of Medicine, 347(3), 161–167. https://doi.org/10.1056/NEJMoa020233
- Januzzi, J. L., et al. (2005). The N-terminal Pro-BNP Investigation of Dyspnea in the Emergency department (PRIDE) study. The American Journal of Cardiology, 95(8), 948–954. https://doi.org/10.1016/j.amjcard.2004.12.032
- Yancy, C. W., et al. (2017). 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure. Journal of the American College of Cardiology, 70(6), 776–803. https://doi.org/10.1016/j.jacc.2017.04.025
- Ibrahim, N. E., & Januzzi, J. L. (2018). Established and Emerging Roles of Cardiac Biomarkers in Heart Failure. Circulation Research, 123(5), 614–629. https://doi.org/10.1161/CIRCRESAHA.118.313215
- Maisel, A., et al. (2008). Less Is More: Impact of NT-proBNP Change Across Hospitalizations in ADHF. Journal of the American College of Cardiology, 51, 1874–1882.
- UpToDate. (2025). Natriuretic peptide measurement in heart failure. Wolters Kluwer. https://www.uptodate.com
- Overview of the management of heart failure with reduced ejection fraction in adults – UpToDate